MediPass: A Pre-Arrival AI Triage and Redirection System to Reduce Emergency Room Overcrowding
Achindra Paul, Reese Lahey
Joane Cardinal-Schubert High School
Grade 11
Presentation
Problem
Alberta is facing a healthcare crisis. Across the province, emergency departments are overwhelmed with patient care. The Alberta Medical Association states "Alberta's overcrowded ER's need system-wide fixes." In January 2026, 242 internal medicine and emergency medicine physicians added their names into a survey to implement practical solutions and put patient safety at the centre of every decision. By January 11 2026, Alberta doctors reported six preventable deaths that occurred due to emergency room wait times. While physician shortage and a rising population affect the issue, a strong contributing factor is the overuse of emergency rooms. 15% of people in any given emergency department are there unnecessarily. That is approximately one in seven people whose issues could be cared for by other specialists.
The main reason why people visit the emergency room unnecessarily is anxiety. Medical anxiety (the excessive persistent worry about having or developing a serious undiagnosed medical condition) is an ongoing concern within the Alberta population. This stems from a variety of societal factors, but mainly from social media. Social media causes phenomena such as cyberchondria, (the obsessive research of symptoms), "doom scrolling," and having constant exposure to health stories. Patients seeking professional reassurance that they are healthy make up 9% of the 15% of unnecessary visits. The remaining 6% of the statistic is made of patients who lack easy access to other divisions of physicians. When a physician's time is occupied with easing concerns or dealing with non-emergent health issues, patients who are suffering from an urgent medical emergency may not receive the help they need in an adequate amount of time.
This poses the question, can a pre-arrival AI triage system using CTAS criteria reduce unnecessary emergency department visits without increasing under-triage risk?
Method
MediPass is an app whose algorithm can triage and filter out patients who seek help unnecessarily before the decision to go to the emergency room is made. When someone is unsure if an emergency room visit is reasonable or if they are simply seeking reassurance they can use MediPass. It will analyze symptoms and health information. It will then, using CTAS, triage the patient. If that patient falls under CTAS 5 the app will give a likely diagnosis and a link to other physicians offices such as family medicine or physiotherapy. If they fall under a higher CTAS ranking the app will advise them to visit the emergency room. The algorithm will mimic the current statistics of medical staff over triage to incorporate human caution. Hypothesis: MediPass will correctly redirect at least 80% of CTAS 5 cases away from emergency departments while maintaining under-triage rates below 5%.
CTAS levels vs MediPass direction: CTAS I: severely ill, requires resuscitation - immediate direction to emergency room CTAS II: requires urgent care and rapid medical intervention - immediate direction to emergency room CTAS III: requires urgent care - emergency care recommendation CTAS IV: requires less-urgent care - urgent care\clinic direction CTAS V: requires non-urgent care - clinic direction or home care recommendations
Medical staff have to take all of one's stated symptoms and factor them into these categories while attempting to avoid under and over triage. Over triage:
- Definition: Patients presenting symptoms that are less severe than they claim, or experiencing anxiety that amplifies trivial issues into perceived emergencies.
- Common Causes: anxiety, lack of primary care access, or in rare cases, secondary gain (malingering).
- Factors Associated with over-triage: younger age (18-30), traumatic injuries, and arrival during evening shifts.
- ED Impact: over-triage is significantly more common than under-triage, with studies showing rates of over-triage around 26% compared to 4.9% for under-triage. This contributes to overcrowding and long wait times.
- Clinical Marker: symptoms that seem more intense or diffuse than expected may be associated with lower ratings of communication effectiveness and trust between patient and provider.
Under-triage:
- Definition: patients downplaying severe, life-threatening symptoms, often due to stoicism, fear, or lack of awareness of the severity.
- Common causes: cognitive decline, cultural factors, or simply not recognizing symptoms as serious.
- Factors associated with under-triage: older age, non-specific or atypical symptoms (e.g., in cardiac patients), and specific complaints like abdominal pain.
- ED impact: While less frequent (4.9% in some studies), under-triage poses a higher risk of morbidity and mortality.
Risk Analysis and Safety Modeling: Risk mitigation strategies:
- Risk override system
- Age-adjusted severity scoring (elderly bias correction)
- Built-in uncertainty threshold (if model confidence <70% → ER)
This system is intentionally biased towards over triage to minimize risk and liability. The system will only give a likely diagnosis if the symptoms fall under CTAS 5 to avoid false reassurance. The risk override system involves the immediate redirection to emergency services if the following symptoms are entered:
- Chest pain
- Unilateral weakness
- Slurred speech
- Neurological deficits
- Severe shortness of breath
Ethical and Legal Framework:
- AI liability: Ai is never 100% accurate and does not incorporate human experience
- Data privacy: MediPass has to abide by the HIA (Alberta Health information act) and PIPEDA (Personal Information Protection and Electronic Documents Act)
- Patients must be able to provide informed consent
- The app must avoid racial, age, and language biases
- The app must avoid the risk of false reassurance
To fulfil these precautions MediPass will consistently enforce a disclaimer, have multiple language options, will not allow disclosure of one's name, address, insurance or other private information a doctor may take, and always suggest professional intervention. MediPass will require a consent form before allowing access to the app. These measures aim to reduce legal and ethical risk.
Official Disclaimer: MediPass cannot replace a medical professional. AI cannot replace human intuition, experience, or life education. Do not take advice with 100% certainty. Medipass should be used as a redirection system and not a diagnostic authority.
Data encryption and security: To ensure patient privacy and comply with healthcare data protection regulations, MediPass would implement multiple layers of security. All data transmitted between the user’s device and the MediPass server would be encrypted using TLS 1.3 (Transport Layer Security). This prevents interception of sensitive health information during transmission. Any health data temporarily stored for analysis would be encrypted using AES-256 encryption, a standard widely used in healthcare and financial systems. All security measures would follow guidelines from Alberta's Health Information Act
Future Implementation: Before real world integration, MediPass would undergo a three-phase validation pilot study, including simulated CTAS case testing, parallel hospital trials with triage nurses, and real-world pilot implementation through Alberta Health Services to ensure clinical safety and reliability. Phase 1: Expand Simulation Method
- Use 500–1000 simulated patient cases
- Cases derived from published CTAS descriptors and anonymized training datasets
- Run all cases through MediPass
Measure
- Sensitivity (correct ER identification)
- Specificity (correct non-ER redirection)
- Under-triage rate (dangerous misses)
- Over-triage rate (safe but inefficient)
Goal Healthcare triage systems aim for:
- Under-triage < 5%
- High sensitivity (>90%)
Phase 2: Controlled Hospital Pilot The next stage would involve testing in collaboration with a hospital or health authority. In Alberta this would likely involve:
- Alberta Health Services
- One emergency department site such as; Foothills Medical Centre or Rockyview General Hospital
Pilot Setup Patients would use MediPass before arriving at the ER. Workflow:
- Patient scans a QR code or downloads MediPass
- They complete the symptom questionnaire
- MediPass gives a recommendation:
- ER
- Urgent care
- Walk-in clinic
- Home care
- When patients arrive at ER, nurses compare:
- MediPass triage prediction
- Actual CTAS triage assigned by nurse
Phase 3: Parallel Testing With Nurses During the pilot, the system does NOT replace nurses. Instead it runs in parallel.
| Step | Process |
|---|---|
| Patient completes MediPass | AI predicts CTAS level |
| Triage nurse assesses patient | Real CTAS assigned |
| Researchers compare results | Measure accuracy |
This allows researchers to calculate:
- AI accuracy
- Missed emergencies
- Over-triage cases
- Time saved
4. Metrics the Pilot Would Track The pilot would measure: Clinical Safety
- Sensitivity
- Specificity
- Under-triage rate
- Over-triage rate
Operational Impact
- Change in ER wait times
- Reduction in non-emergent visits
- Patient satisfaction
Economic Impact
-
Cost savings for Alberta healthcare
Ethics and Data Security During the Pilot
The study would require approval from a research ethics board such as:
- University of Calgary Conjoint Health Research Ethics Board
All patient data would:
- Be anonymized
- Be encrypted (TLS + AES-256)
- Not store identifying health information
6. Small Scale Pilot Timeline Example timeline students could present:
| Stage | Duration |
|---|---|
| Simulation testing | 2 months |
| Hospital pilot preparation | 1 month |
| Live pilot testing | 3 months |
| Data analysis | 1 month |
Total: \~7 months Starting a trial in one local hospital will allow a gauge for success and identify elements in need of improvement. Additionally to the pilot study a behavioral psychology study to assess medical anxiety before and after use, and compare reassurance vs escalation behavior. Then proceed to broaden its use by displaying posters with QR codes in medical facilities and integrate it within the Alberta health services app.
Limitations:
- MediPass has not been clinically trialed
- Has a simulated dataset (no real people were used in testing) - a larger dataset with real clinical data would improve liability
- The app cannot asses physical examination cues such as blood pressure or oxygen levels the same as a triage nurse can
- Risk of misuse - patients may inaccurately describe their symptoms
Machine Learning / Artificial Intelligence
MediPass will use Artificial Intelligence (AI) and Machine Learning (ML) to analyze patient symptoms before they arrive at the hospital and predict the urgency of their condition in real time. AI refers to computer systems that simulate human decision-making, while machine learning is a subset of AI that allows systems to learn patterns from data and improve over time without being explicitly reprogrammed. When a patient enters their symptoms into the MediPass app, the system collects structured data such as:
- Age and gender
- Presenting symptoms
- Pain severity (1–10 scale)
- Duration of symptoms
- Pre-existing medical conditions
- Vital signs (if available)
Because the available dataset was limited, MediPass used a hybrid prototype system combining rule-based CTAS logic with a simplified decision-tree classification model. The simulated dataset was used to test the decision logic rather than fully train a large-scale machine learning system.. Instead of simply matching keywords, the AI analyzes combinations of symptoms and risk factors to detect patterns that may indicate serious conditions. The system will also include an AI-powered chatbot interface that:
- Asks follow-up questions
- Clarifies symptom severity
- Ensures complete information is gathered
- Provides understandable recommendations
For non-urgent cases, MediPass can suggest alternative care options such as walk-in clinics, virtual consultations, or pharmacies. For urgent cases, it can advise immediate hospital visits and notify emergency departments in advance. Over time, the system improves by learning from real patient outcomes. For example, if a patient classified as “urgent” was later admitted to intensive care, the model adjusts its internal parameters to better recognize similar future cases. This continuous learning process increases prediction accuracy and reliability.
// Example patient input
let patient = {
age: 68,
chestPain: true,
difficultyBreathing: true,
fever: false,
painLevel: 8
};
// Simple probability calculation
let emergencyProbability = 0;
if (patient.chestPain) {
emergencyProbability += 40;
}
if (patient.difficultyBreathing) {
emergencyProbability += 40;
}
if (patient.age > 65) {
emergencyProbability += 20;
}
console.log("Emergency Probability:", emergencyProbability + "%");
Classification in Artificial Intelligence
MediPass will use classification algorithms, a type of supervised machine learning, to sort patients into predefined categories based on symptom data and medical history. The primary categories may include:
- Emergency
- Urgent
- Non-Urgent
Classification works by training the model on historical patient datasets that include both symptom data and confirmed medical outcomes. Because the outcomes are already known, this is called supervised learning. The system learns patterns such as:
- Certain symptom clusters being strongly associated with hospital admission
- Specific age groups having higher risk for certain conditions
- Combinations of symptoms that frequently result in emergency intervention
Possible classification models could include:
- Decision Trees
- Random Forest
- Logistic Regression
- Neural Networks
Each model analyzes input variables and assigns a probability score to each category. The category with the highest probability becomes the final classification. This classification system helps reduce emergency department overcrowding by safely redirecting non-urgent cases while prioritizing high-risk patients who require immediate attention.Decision Trees were selected because they provide transparent decision logic, which is important in healthcare AI where explainability and accountability are required.
function classifyPatient(score) {
if (score >= 70) {
return "Emergency";
} else if (score >= 40) {
return "Urgent";
} else {
return "Non-Urgent";
}
}
let classification = classifyPatient(emergencyProbability);
console.log("Classification:", classification);
Rule-Based Systems
In addition to machine learning, MediPass will incorporate a rule-based expert system to ensure safety and consistency. Rule-based systems operate using predefined “if–then” logic derived from established medical triage guidelines. Examples include:
- If chest pain AND difficulty breathing → classify as emergency
- If high fever in child under 2 years old → urgent
- If severe bleeding → emergency
- If mild sore throat with no fever → non-urgent
Rule-based systems are especially important for critical red-flag symptoms because they guarantee that certain dangerous conditions are never ignored due to statistical probability. This hybrid approach — combining rule-based logic with machine learning — strengthens the system by:
- Ensuring consistent safety standards
- Reducing false negatives (missing real emergencies)
- Providing transparent decision explanations
- Supporting ethical AI use in healthcare
By using both systems together, MediPass balances predictive intelligence with strict medical safeguards.
function ruleBasedCheck(patient) {
if (patient.chestPain && patient.difficultyBreathing) {
return "Emergency - Call 911 Immediately";
}
if (patient.fever && patient.age < 2) {
return "Urgent - Seek Medical Attention";
}
return "No Critical Rule Triggered";
}
let ruleResult = ruleBasedCheck(patient);
console.log(ruleResult);
Feature Engineering
Feature engineering is a crucial step in improving the performance of AI models. It involves transforming raw patient data into meaningful numerical values that can be effectively analyzed by machine learning algorithms. Raw data alone is not always sufficient. For example:
- “Chest pain” must be converted into a severity level
- “Age 75” must be interpreted as higher cardiovascular risk
- “Diabetes + infection” may indicate increased complication risk
Through feature engineering, MediPass can create:
- Symptom severity scores
- Risk multipliers based on age
- Comorbidity risk indexes
- Time-based progression factors (longer duration = higher risk)
- Vital sign abnormality indicators
For example, heart rate above normal range could be converted into a binary feature (normal/abnormal) or a scaled deviation score. Well-designed features allow the model to:
- Detect complex relationships
- Improve prediction accuracy
- Reduce misclassification
- Increase reliability in edge cases
Feature engineering is often one of the most important components of building an effective healthcare AI system.
function createFeatures(patient) {
let features = {};
// Age risk factor
features.ageRisk = patient.age > 65 ? 20 : 5;
// Symptom severity score
features.severityScore = patient.painLevel * 5;
// Binary feature (true = 1, false = 0)
features.breathingRisk = patient.difficultyBreathing ? 30 : 0;
return features;
}
let engineeredFeatures = createFeatures(patient);
console.log(engineeredFeatures);
Risk Scoring
MediPass will implement a risk scoring system that assigns each patient a numerical value representing the severity of their condition. Rather than simply labeling someone as urgent or non-urgent, the system calculates a weighted score based on:
- Symptom severity
- Age-related risk factors
- Medical history
- Presence of high-risk conditions
- Abnormal vital signs
For example: Risk Score = (Symptom Severity × Symptom Weight) + (Age Risk Factor) + (Comorbidity Score) + (Vital Sign Abnormality Index) The final score could fall within a defined scale, such as:
- 0–30 → Low Risk
- 31–70 → Moderate Risk
- 71–100 → High Risk
Risk scoring offers several advantages:
- Provides a clear, explainable numerical output
- Allows flexible decision thresholds
- Helps hospitals prioritize incoming patients
- Supports dashboard visualization for administrators
Most importantly, it ensures that high-risk patients are identified quickly and directed to immediate care.
function calculateRiskScore(features) {
let totalScore = 0;
totalScore += features.ageRisk;
totalScore += features.severityScore;
totalScore += features.breathingRisk;
return totalScore;
}
let riskScore = calculateRiskScore(engineeredFeatures);
console.log("Final Risk Score:", riskScore);
// then classify based on risk
let finalDecision = classifyPatient(riskScore);
console.log("Final Decision:", finalDecision);
// how the result will be shown
let features = createFeatures(patient);
let score = calculateRiskScore(features);
let decision = classifyPatient(score);
console.log("Patient Triage Result:", decision);
MediPass Algorithm Overview
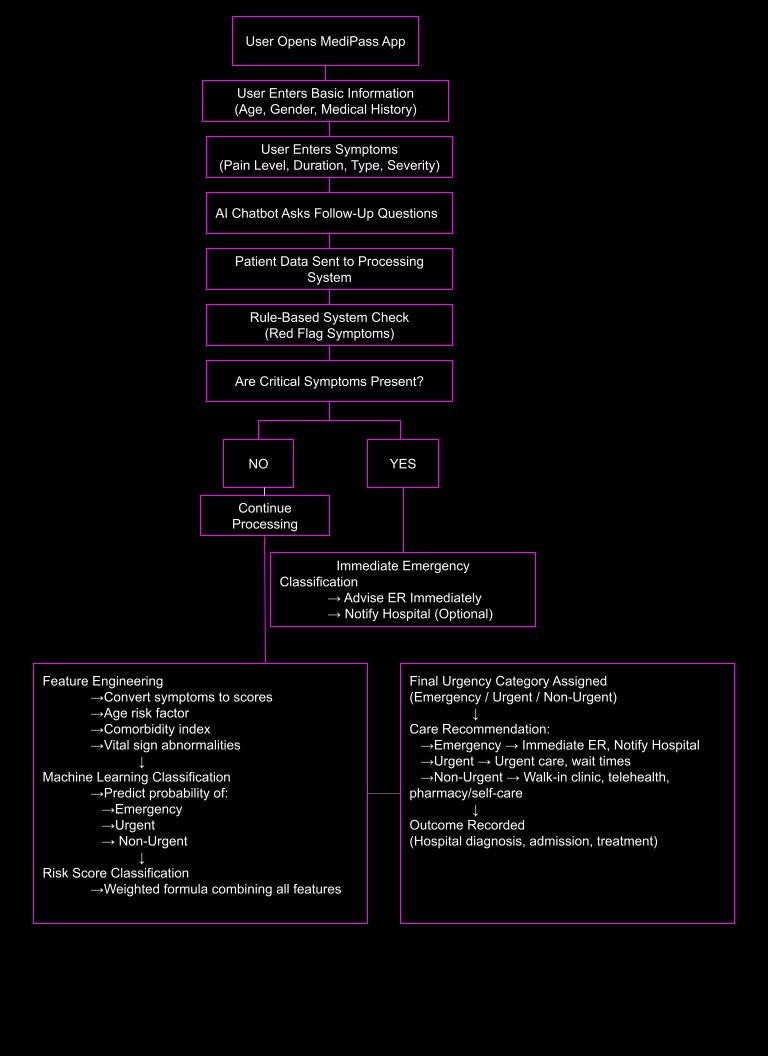
The MediPass system is designed to efficiently evaluate patient symptoms and health information, predict urgency levels, and guide care decisions in a safe, reliable way. The algorithm combines feature engineering, rule-based safety checks, and machine learning classification to produce accurate recommendations.
Step 1: Patient Inputs
Patients enter their symptoms and health information through the app, including:
- Age and gender
- Symptom description
- Pain severity (1–10 scale)
- Symptom duration
- Pre-existing conditions
- Vital indicators (if available, e.g., heart rate, temperature)
This raw data forms the foundation of the analysis.
Step 2: Feature Engineering
The system converts raw inputs into numerical features that the machine learning model can understand. Examples include:
- Symptom severity score (weighted by symptom type)
- Risk score based on comorbidities or chronic conditions
- Age-based risk modifier
- Vital sign deviation scores
- Symptom progression factor (longer duration → higher risk)
These engineered features allow the model to capture meaningful relationships between symptoms, patient history, and urgency.
Step 3: Rule-Based Safety Filter
Before any machine learning prediction occurs, a rule-based CTAS (Canadian Triage and Acuity Scale) safety filter runs.
- Ensures that critical “red-flag” symptoms (e.g., chest pain, shortness of breath, stroke symptoms) automatically trigger emergency recommendations.
- Guarantees safety and consistency, preventing the model from misclassifying life-threatening cases.
This hybrid approach balances predictive intelligence with strict medical safeguards.
Step 4: Machine Learning Model Classification
MediPass uses a Decision Tree classifier as the primary machine learning model.
- The model predicts the urgency level based on the engineered features.
- Possible output categories:
- Emergency / ER
- Urgent Care
- Clinic Visit
- Home Care
Why Decision Tree?
- Simple to interpret and visualize
- Performs well with structured, tabular data
- Works efficiently for a student project while demonstrating real AI principles
- Can be combined with rule-based safety checks for hybrid accuracy
Step 5: Confidence Threshold
The system applies a confidence threshold to the model’s prediction:
- If the model is highly confident, the recommendation is used directly.
- If the confidence is low, the system may escalate to a higher safety level or suggest additional assessment questions.
This ensures that recommendations are reliable and explainable.
Step 6: Final Care Recommendation
Based on the combination of the rule-based filter, Decision Tree prediction, and risk scoring, MediPass outputs a final care recommendation:
- Emergency → go to ER immediately
- Urgent Care → visit urgent care clinic soon
- Clinic → schedule standard appointment
- Home Care → self-manage with instructions
These recommendations are presented clearly to the patient and optionally shared with hospital staff for prioritization.
MediPass Data Pipeline
Input Data
- Age
- Symptoms
- Pain level
- Symptom duration
- Medical history
- Vital indicators
↓ Feature Engineering
- Symptom severity score
- Risk score
- Age risk modifier
- Vital sign deviation
- Symptom progression factor
↓ Model Classification
- Decision Tree predicts urgency level:
- ER
- Urgent Care
- Clinic
- Home Care
↓ Safety Layer / Rule-Based CTAS Filter
- Confidence threshold check
- Critical symptom override ensures safety
↓ Output
- Final care recommendation
- Optional hospital dashboard notification
Analysis
Accuracy Analysis: A synthetic dataset of 100 simulated patients was created using published CTAS case descriptors, used for training purposes. Each case included age, symptoms, duration, and severity. Cases were proportionally distributed according to CTAS provincial averages (decimal places were rounded for experimental purposes). The dataset was used to evaluate the decision model rather than to fully train a large-scale machine learning system. The following statistics were produced:
- Sensitivity (ER cases correctly identified) 91%
- Specificity (non-ER correctly redirected) 83%
- Over triage safety margin 15%
- Under-triage rate of 3%, mostly due to lack of specificity of patients leading to broader suggestions Classification breakdown:
- Predicted E.R cases: 66
- Actual E.R cases: 72
- Predicted non E.R cases: 24
- Actual non E.R cases: 29
- Cases misidentified (over-triage): 7
- Cases misidentified (under-triage):3
CTAS provincial averages: CTAS 1: 1.3% CTAS 2: 18.0% CTAS 3: 52.2% CTAS 4: 25.9% CTAS 5: 2.3%
Case Walkthrough Example: Patient downloads MediPass They read and indicate the consent form Patient enters basic information (age 22, language English) They enter stomach pain as main concern with 4-5 day duration Patient enters stomach pain and chest tightness for symptoms Patient enters none for previous disease or conditions Patient enters 4/moderate for pain level Patient enters regular mental health, heart rate, and breathing, with a slight fever MediPass triaged into CTAS 2 Recommended patient go to the emergency room in 15 minutes and gave a link to call 911
Cost Benefit Analysis: The average non-emergent emergency department visit costs $361. In Alberta, in 2025 there were an estimated 725,000 emergency room visits. If 15% of those visits were non-emergent, $39,258,750 was spent. If MediPass can reduce 5% of non-emergent visits the Alberta government would save $1.96 million annually.
Future Accessibility Improvement: In the testing phase of the accuracy analysis and phase one of the pilot study, medical language is widely understood by researchers. Issues may arise when real patients with less fluency in medical knowledge attempt to describe their symptoms. A way MedIpass will try to avoid this issue is showing visual representation. Pictures that describe different types of headaches, what a fever is, how to take one's temperature, and other images that help explain how to properly fill out MediPass's questionnaire.
Conclusion
MediPass met its hypothesis when the prototype system achieved 91% sensitivity in identifying emergency cases and 83% specificity in redirecting non-emergency cases, while maintaining an under-triage rate of 3%. These results suggest that an AI-assisted pre-arrival triage system could reduce unnecessary ER visits while maintaining patient safety. MediPass is projected to save $1.96 million annually in Alberta. The app will likely take 7 months to deploy and based on overcrowding reduction statistics found in the pilot study could continue to hold importance in the future. With real world integration MediPass would likely be able to reduce emergency room overcrowding in Alberta without increasing under-triage risks, while saving money and reducing load on emergency care physicians.
Citations
Canadian Association of Emergency Physicians (CAEP) & CTAS National Working Group (NWG). (2012). THE CANADIAN TRIAGE AND ACUITY SCALE Combined Adult/Paediatric Educational Program PARTICIPANT’S MANUAL. In Triage Training Resources (Version 2.5b, November 2013). https://ctas-phctas.ca/wp-content/uploads/2018/05/participant_manual_v2.5b_november_2013_0.pdf
Lupton, J. R., Davis-O’Reilly, C., Jungbauer, R. M., Newgard, C. D., Fallat, M. E., Brown, J. B., Mann, N. C., Jurkovich, G. J., Bulger, E., Gestring, M. L., Lerner, E. B., Chou, R., & Totten, A. M. (2022). Under-Triage and Over-Triage Using the field Triage Guidelines for Injured patients: A Systematic review. Prehospital Emergency Care, 27(1), 38–45. https://doi.org/10.1080/10903127.2022.2043963
Health Information Act. (2026, February 12). Alberta.ca. https://www.alberta.ca/health-information-act
Legislative Services Branch. (2025, March 4). Consolidated federal laws of Canada, Personal Information Protection and Electronic Documents Act. https://laws-lois.justice.gc.ca/eng/acts/p-8.6/
Ontario Psychological Association - What’s the connection between social media and mental health? (n.d.). https://www.psych.on.ca/Public/Blog/2023/Shades-of-Blue-How-Different-Types-of-Depressi-(5)#:\~:text=Social%20media%20may%20enhance%20other,for%20your%20smartphone%20too%20frequently.
Total hourly number of emergency visits for patients residing in the local geographic area for triage levels Semi-Urgent(4) and Non-Urgent(5) combined, by Weekday/Weekend, Fiscal year 2023/2024 - Open Government. (n.d.). https://open.alberta.ca/opendata/all-emergency-visit-for-patients-residing-in-the-local-geographic-area-lga-for-triage-levels
Society of Rural Physicians of Canada. (2014). THE CANADIAN PREHOSPITAL ACUITY SCALE Educational Program PARTICIPANT’S MANUAL. https://ctas-phctas.ca/wp-content/uploads/2018/05/pre-ctas_manual_2014_v1.5.pdf
Savulescu, J., Giubilini, A., Vandersluis, R., & Mishra, A. (2024). Ethics of artificial intelligence in medicine. Singapore Medical Journal, 65(3), 150–158. https://doi.org/10.4103/singaporemedj.smj-2023-279
O’Cathain, A., Connell, J., Long, J., & Coster, J. (2019). ‘Clinically unnecessary’ use of emergency and urgent care: A realist review of patients’ decision making. Health Expectations, 23(1), 19–40. https://doi.org/10.1111/hex.12995
AMA Report Card on the state of health care in Alberta | AMA. (2025, July 4). https://www.albertadoctors.org/news/publications/presidents-letter/ama-report-card-on-the-state-of-health-care-in-alberta/
No answer to our SOS | AMA. (2024, August 27). https://www.albertadoctors.org/news/publications/presidents-letter/no-answer-to-our-sos/
Alberta Health Services. (2021). Alberta Health Services Annual Report Supplementary information. In Alberta Health Services Annual Report (p. 28). https://www.albertahealthservices.ca/assets/about/publications/ahs-pub-pr-2021-22-q4-objective-08-hospital-stay.pdf
Sartini, M., Carbone, A., Demartini, A., Giribone, L., Oliva, M., Spagnolo, A. M., Cremonesi, P., Canale, F., & Cristina, M. L. (2022). Overcrowding in Emergency Department: Causes, Consequences, and Solutions—A Narrative Review. Healthcare, 10(9), 1625. https://doi.org/10.3390/healthcare10091625
Artificial Intelligence & Basics
IBM Cloud. (n.d.). What is artificial intelligence (AI)? https://www.ibm.com/cloud/learn/what-is-artificial-intelligence
McKinsey Global Institute. (2018). Notes from the AI frontier: Applications and value of deep learning. https://www.mckinsey.com/featured-insights/artificial-intelligence
Russell, S., & Norvig, P. (2010). Artificial intelligence: A modern approach (3rd ed.). Pearson.
Types of AI
Future of Life Institute. (n.d.). Artificial general intelligence (AGI) and superintelligence. https://futureoflife.org/background/aim/
Russell, S., & Norvig, P. (2010). Artificial intelligence: A modern approach (3rd ed.). Pearson.
Machine Learning Overview
Google Developers. (n.d.). Machine learning crash course. https://developers.google.com/machine-learning/crash-course/ml-intro
Mitchell, T. (1997). Machine learning. McGraw Hill.
Scikit-learn. (n.d.). Supervised learning. https://scikit-learn.org/stable/tutorial/statistical_inference/supervised_learning.html
Supervised, Unsupervised, and Reinforcement Learning
Sutton, R., & Barto, A. (2018). Reinforcement learning: An introduction (2nd ed.). MIT Press. https://web.stanford.edu/class/psych209/Readings/SuttonBartoIPRLBook1stEd.pdf
Scikit-learn. (n.d.). Clustering (unsupervised learning). https://scikit-learn.org/stable/modules/clustering.html
Classification & ML Algorithms
Brownlee, J. (2020). Types of classification in machine learning. Machine Learning Mastery. https://machinelearningmastery.com/types-of-classification-in-machine-learning/
Scikit-learn. (n.d.). Supervised learning models. https://scikit-learn.org/stable/user_guide.html#supervised-learning
Feature Engineering
Kaggle. (n.d.). Feature engineering. https://www.kaggle.com/learn/feature-engineering
Kuhn, M., & Johnson, K. (2019). Feature engineering and selection: A practical approach for predictive models. CRC Press.
Risk Scoring
PubMed. (n.d.). Risk scoring in healthcare using machine learning. https://pubmed.ncbi.nlm.nih.gov/?term=risk+scoring+machine+learning
Brownlee, J. (2016). Probability-based and binary risk scoring in ML. Machine Learning Mastery. https://machinelearningmastery.com
Rule-Based Systems & Expert Systems
Russell, S., & Norvig, P. (2010). Artificial intelligence: A modern approach (3rd ed.). Pearson.
TutorialsPoint. (n.d.). Expert systems tutorial. https://www.tutorialspoint.com/expert_systems/index.htm
Acknowledgement
We would like to acknowledge the use of Base44 AI to assist in creating code, and helping create a platform for the app model. The use of ChatGPT to assist in grammar corrections, and helping get a structure for how the project format could be completed. The support provided from our teacher, Ms Sung, her advice, guidance and technical assistance was impactful on our ability to complete this project. Nirvana Ahmed for turning our concept art into digital art for our display. Lastly the inputs and perspectives from ward one council woman Kim Tyers, Ms Esther Li, Dr Gillian Stewart, and Amy Muller. We could not have achieved our ambitions with this project without their personal experience.