
ClotGuard: Autonomous Hemostatic Treatment (Co-Founded with Sophia Dhami)
Isavella Tsoulias
Queen Elizabeth High School
Grade 10
Presentation
Problem
Background on Deaths Due to Hemorrhage
Hemorrhage, or uncontrolled bleeding, is a major cause of preventable deaths, especially when the body is affected by traumatic injuries. It’s estimated that hemorrhage accounts for 1.5 million global deaths every year, while excessive blood loss in injuries accounts for roughly 2 million deaths each year, for civilian-related accidents. This ends up costing more than $670 billion a year for treatment and resources. On the battlefield, roughly 81.5% of fatalities were due to hemorrhage, and all fatalities occurred before the casualties reached a medical facility. Around 80% of Potentially Survivable (PS) ‘Died of Wounds’ (DOW) deaths on the battlefield were caused by hemorrhage from major trauma.
Background on Hemorrhage
It takes roughly 2-5 minutes for a hemorrhage to become deadly (bleed to death) and roughly 7-10 minutes for paramedics to arrive on scene to treat. Because of these statistics, we found that the treatment we give to hemorrhage patients isn't the problem; it's the amount of time it takes for them to receive life-saving care that creates these preventable deaths. That's why we resort to using methods such as gauze, tourniquets, and injectables on site as an attempt to slow bleeding.
Current Solutions
The first concern with these methods of preliminary treatment is that we don't see these death statistics changing. This is a sign that we need a new method for managing hemorrhage on-site more effectively. There are other problems with current treatment methods:
- They're too expensive (the US military spent $8.2 billion on medical supplies)
- They're too hard to clean up after
- They don't work well for irregular wound types
 Another important concern with these treatment supplies is that they are non-autonomous, meaning that they need at least one person to help deliver these solutions, which is impractical in high-stress situations and wastes time, which can be the reason a trauma injury turns fatal.
Another important concern with these treatment supplies is that they are non-autonomous, meaning that they need at least one person to help deliver these solutions, which is impractical in high-stress situations and wastes time, which can be the reason a trauma injury turns fatal.
Other solutions, like the deployment of Forward Surgical Teams (FSTs) has been a key military response to delayed trauma care times. These are compact, mobile medical units made to be placed near areas of conflict. This includes 20 people, including nurses, medics, anesthetists, and surgeons.
- Speed: After reaching the location, it can be completely functional in approximately 90 minutes.
- Purpose: The goal is to perform damage control surgery, which is a crucial intervention that keeps a patient stable long enough to survive evacuation.
According to a U.S. Army Medical Department report, “the goal of an FST is not definitive care, but survival.”
When compared to earlier models that postponed surgery until hospital arrival, their presence has raised survival rates by as much as 25% in certain operations. FSTs still have to deal with issues like scarce resources and the ongoing danger of enemy fire, which can reduce their efficacy. Despite being a significant advancement in battlefield trauma care, forward surgical teams still have significant flaws in their design that result in preventable deaths.
- Limited Resources: Due to their incredibly light design, FSTs are unable to perform complicated surgeries or care for several critically ill patients at once. According to a USAMD report, an FST can usually only handle two to three surgeries at once before becoming overburdened. Even after arriving at the FST, many soldiers are still required to wait an excessive amount of time for care during mass casualty incidents.
- Short Operating Window: FSTs typically need resupply or evacuation support after operating for less than 72 hours. Due to the lack of ICU-level support provided by FSTs, injured soldiers may rapidly deteriorate if evacuation aircraft are delayed even slightly.
- Fragile and Vulnerable: FSTs are frequently high-risk targets themselves because of their proximity to the frontline. Teams occasionally have to leave patients behind and relocate rapidly under fire in unstable areas, leaving unfinished treatments in their wake. 10% of FST relocations in Afghanistan were “emergency withdrawals under enemy pressure,” according to a Pentagon report, further endangering lives.
- Employee Fatigue and Burnout: FSTs typically have a very small number of nurses and surgeons who are expected to manage a high volume of trauma cases in a demanding environment. A RAND study found that after only 48 hours of nonstop work, medical staff in FSTs experienced “severe mental and physical exhaustion.” This fatigue raises the risk of fatal miscalculations, incorrect amputations, and medical errors.
- Evacuation Dependency: FSTs solely depend on fast MEDEVAC to get stabilized patients to full hospitals after initial surgery. Delayed air support leaves injured soldiers trapped in facilities, unable to carry on lifesaving therapy, therefore causing unnecessary death in the process.
Another solution in action and further progress is the creation of Mobile Trauma Bays (MTBS), which are like tiny emergency rooms on wheels. Mounted on military vehicles or mobile platforms, they are ready to give quick, critical care right at or near the point of injury. Usually manned by one physician, one nurse, and several corpsmen. In some situations, MTBS have reached a high survival rate for those injured (Marines) who received early treatment within them. They can avoid delays connected with waiting for MEDEVAC helicopters by moving alongside troops. A piece in the U.S. Navy Medical Corps said: Rolling out trauma treatment right away at the site of injury changed the equation from ‘time to care’ to ‘care time at zero.’ When weather, enemy control, airspace, or distance preclude rapid air evacuation, this “ER on the move” idea becomes crucial.
While Mobile Trauma Bays sound revolutionary, they have major drawbacks. They are heavily limited in capacity, often treating only one or two critical patients at a time, and lack the full surgical capabilities of a hospital or even an FST. In intense combat scenarios, overcrowding and equipment shortages can quickly overwhelm them, and their mobility can be restricted by rough terrain or enemy fire.
An additional solution gaining attention is DARPA’s “Golden Hour” Evacuation program, which aims to create autonomous aircraft that can rapidly evacuate wounded soldiers from the battlefield. The idea is to remove the delays caused by waiting for human pilots or medevac teams. However, while promising in theory, the project has faced major hurdles. Autonomous aircraft still struggle with navigation in hostile, unpredictable environments, especially where enemy fire, GPS jamming, and rugged terrain are involved. Not to mention, trusting a fully robotic system with the lives of critically injured soldiers feels like a huge gamble to many in the military community. As of now, DARPA’s vision remains mostly experimental and nowhere close to full battlefield deployment, leaving today’s wounded still heavily dependent on traditional, slower evacuation methods.
The military is also experimenting with drones and AI to speed up trauma care. Drones are being tested for faster delivery of blood, medical supplies, and even lightweight evacuation options to troops in hard-to-reach areas. AI is being developed to triage injuries, predict medical deterioration, and even assist field medics with decision-making. But despite the flashy headlines, these technologies bring a lot of baggage. Drones can be shot down or malfunction in bad weather, and AI algorithms still have serious biases and reliability issues when operating in the chaos of combat.
One RAND report warned that AI triage systems currently misclassify battlefield injuries about 20% of the time, a mistake rate that could easily mean life or death.
In short, while drones and AI could eventually help, they are not a silver bullet today, and relying on them too soon could actually create new layers of risk for wounded soldiers waiting for urgent help.
Method
ClotGuard Overview
Sophia Dhami, co-founder of ClotGuard, and I aimed to develop a solution to preventable deaths on the battlefield that would fulfill two main requirements:
- Autonomous function: wouldn't require external intervention to be issued
- Quick application: would take under a minute to be administered and functioning to stay within the 2-5 minute threshold
This led us to develop ClotGuard, an autonomous hemostatic patch treatment that autonomously delivers lyophillized platelets to a site of bleeding via nanocarriers to stimulate clot formation and subside bleeding until paramedics arrive.
Step-by-Step Walkthrough of ClotGuard
ClotGuard is a multi-component device, meaning that it has multiple technologies working together as one cohesive system. ClotGuard has 3 main components:
- Patch storage and tracking
- Lyophilized platelet payload
- Nanocarrier transportation
To make sure that this idea was still viable despite the complexity of the device, we made sure to validate and work with experts during each step of the ideation process. The next few sections will walk through exactly how ClotGuard works and the technical validation behind each component.
Detecting the Injury: Patch/Storage
ClotGuard is based on diabetes patches and Continuous Glucose Monitoring (CGM) systems, such as the Dexcom G7 or the Omnipod, but having the two devices combined since the payload is on a smaller scale and for one-time use. The patch is going to track five different biomarkers:
- Systolic Blood Pressure (SBP)
- Concerning level: <100 mmHg
- Strong hemorrhage indicator: <90 mmHg
- Heart Rate (HR)
- Concerning level: >100-110 bpm
- Strong hemorrhage indicator: >120 bpm
- Oxygen Saturation
- Concerning level: <94%
- Strong hemorrhage indicator: <90%
- Blood Velocity
- >20-30% drop from baseline
- Shock Index (HR/SBP)
- Concerning level: ≥0.9
- Strong hemorrhage indicator: ≥1.0
The patch would establish a baseline upon deployment and then monitor the changes from the baseline, this makes it more accurate to each individual. A lot of these are already able to be monitored on existing smart watches using Photoplethysmography (PPG) and ECG electrodes technology, making building the sensors relatively easy to do and already validated. The patch would have to detect 5/5 of the sensors, with shock detection being the most important (weighing in two of the biomarkers, HR and SBP).
At the bottom of the patch, microneedles holding the lyophillized platelets payload will release the payload into the bloodstream on command when all five of the biomarker levels are met.

Patch design for ClotGuard
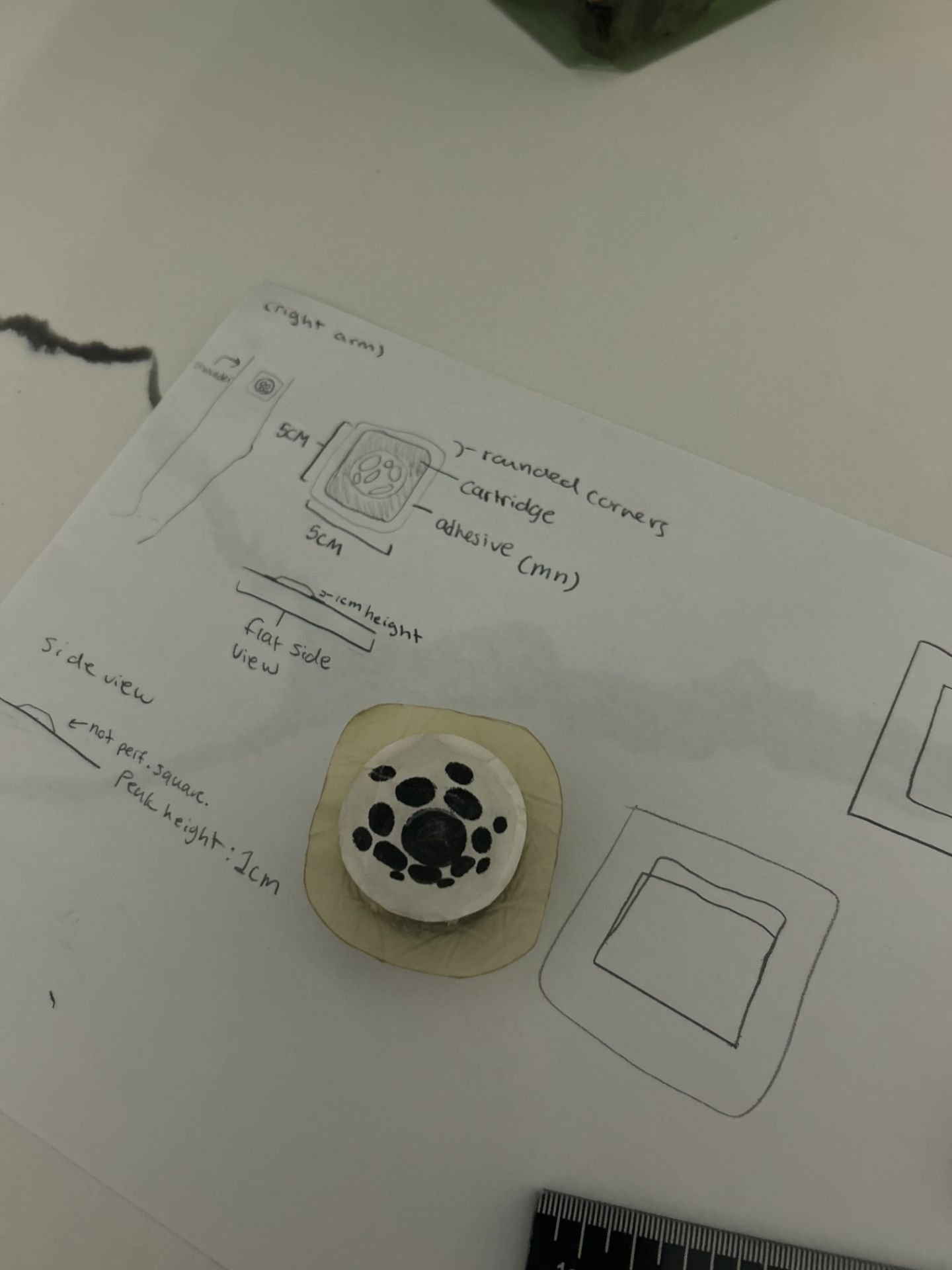 Real life v0 patch design (for visuals only)
Real life v0 patch design (for visuals only)
Payload: Lyophilized Platelets
Inside the microneedles of the patch is where the actual payload that will treat the hemorrhage site is being stored. This payload is a combination of the lyophilized platelets and nanocarriers. The freeze-dried platelets and nanocarriers are "glued" together with linker molecules that degrade in changes in environments (lower pH levels for ClotGuard case). The freeze-dried platelets are going to be synthetic platelets that we develop and test in the lab. There are a couple of reasons why we chose to use synthetic platelets:
- They can be used universally (avoids the issue with blood typing)
- More customizable (can change clotting and speed factors for ClotGuard case)
- Can be hydrated right away, but activated at the specific location
The synthetic platelets are going to be lyophilized (freeze-dried) to ensure that they can be preserved in unpredictable environments for longer periods of time. A study found that lyophilized platelets can be stored at room temperature (20-24℃) for up to 3 years and can be reconstructed in minutes for quick treatment. These lyophilized platelets will then be encapsulated in a thrombin-activated, cleavable peptide coating. This coating has a few components to it:
- Allows the platelets to rehydrate, but they will not activate until they reach the site of bleeding and react to site-specific biomarkers
- Coating is cleaved by thrombin, causing the coating to fall apart and release the platelet to rehydrate and begin clot formation
- Fibrin helps to weaken the layer and acts as a percaussionary trigger
All of these triggers were chosen based on what happens at a trauma site. High fibrin levels can be found at a trauma site quickly and are likely to cause weakening in the coating structure. Thrombin is a fibris protein that can be found in high amounts in early stages of bleeding and is highly specific and localized to the bleeding region, making it an optimal choice for coating cleavability. Once the platelets are released, they will rehydrate and interact wth other platelets and the wound site to begin reinforced clot formation.
Nanocarriers
Our nanocarriers are going to be made out of a bio-safe biopolymer called Poly(lactic-co-glycolic acid) (PLGA) that is widely tested and already FDA approved for treatment use. They are going to locate the site of bleeding through passive flow throughout the bloodstream until it passes the site of bleeding. We are researching utilizing enzyme-based propulsion, which is a technique that is able to autonomously speed up the nanocarriers by creating micro reactions between a specific biomarker (calcium ions, for example) and the enzymes, which end up propelling the nanocarriers in the direction of bleeding. Once the nanocarriers reach the site of bleeding, they will bind to an exposed fibris protein called exposed collagen, which is the first produced protein during hemorrhage that can be found along the lining of the wound, making it an accurate binding spot, preventing the nanocarriers from travelling further in the bloodstream or releasing the platelets in a different area. Once the payload is released, the nanocarriers will begin to degrade and will exit the body within a couple of days.
Testing Roadmap
| Phase | What we are testing | Why |
|---|---|---|
| 1 | Rehydration kinetics and morphology |
|
| 2 | Aggregation/thrombin generation/simple clot mechanics |
|
| 3 | Encapsulation candidates and rationale |
|
| 4 | Patch sensors and storage of payload |
|
| 5 | Nanobot delivery and accuracy |
|
Analysis
While in the ideation phase for ClotGuard, our focus was on a few primary things:
- Gaining advisors to validate the technical/business case for ClotGuard
- Securing collaborations/partnerships
- Finding funding opportunities
- Networking and publicity opportunities
Validation and Advisors
One of the things that makes ClotGuard technically sound is that we've talked to a lot of people about every component of our project for things like technical components, FDA, IP, competitors, and market size. Here is a list of all the advisors we've gathered:
Michael Serpe - University of Alberta at Gunning/Lemieux Chemistry Centre Got the opportunity to tour the Gunning/Lemieux Chemistry Centre, led by Michael Serpe, who was very interested in what we were developing at ClotGuard, as well as our earliest validator/supporter. We specifically reached out to discuss the dissolvable microneedle and PLGA nanoparticle technologies he was developing in his lab. We established having him as an advisor as well as a future collaborator once we begin active testing.
Ejaife Agbani - University of Calgary Met with Ejaife Agbani to discuss the hemostasis and platelet components of ClotGuard. He gave us some guidance on how to proceed with future testing (like different literature reviews and papers to read).
Sara Akbarzadeh - Medical Wearables Reviewer at the FDA Sara met with us to review the theoretical idea for ClotGuard and gave us an overview of the FDA approval process for a device like ours (labelled a class 2 combination device). She validated our idea from an FDA perspective, and she also gave us a rough timeline and asked us to stay updated with our progress.
Noah Smith - IP Analyst at Front Row Ventures Gave him an overview of the idea for ClotGuard and discussed what IP would look like in the future. He gave us a roadmap for the IP process and when we should begin it. We also discussed future collaboration with Front Row Ventures once we are eligible (of age) for funding.
Jeff Ryzner - University of Calgary at the Hunter Hub for Entrepreneurial Thinking Met with Jeff Ryzner to discuss lab opportunities to begin the testing portion for ClotGuard. He was extremely excited about working with us and was determined to help us in any way possible. He connected us to Paula Berton, who would guide us through the actual testing process. He is an advisor for ClotGuard and is able to get us future connections/resources.
Paula Berton - University of Calgary Paula Berton is our connection at the University of Calgary, who can help us in the direct testing process by guiding us on our testing roadmap, delegating and planning the different phases of testing and the components/protocols, as well as helping us secure resources like lab space, funding, and support for testing.
Pablo Guzman - Material Science at A&M Texas Pablo Guzman is helping us with validating the material science components of ClotGuard, as well as helping us with some of the design of the different mechanisms we are using, such as the storage/delivery methods. He validated ClotGuard and said that the process makes sense and logically works, and he asked to keep getting updates from us as we progress.
Alexandra Ramadan - X, The Moonshot Factory Alexandra Ramadan first helped us with ClotGuard when she judged our project at the TKS Moonshots Presentations, where she gave a lot of good feedback about our idea and found it very interesting. Recently, we connected with her again to update her on what we’re working on for ClotGuard and some of the support we’re looking for. She asked us to keep her updated and also send over some of the labs we are looking to work on so she can see if anything would work for us. She validated our idea, especially how much it had progressed since the initial judging she did for it.
Cindy Hui - AtlaML Cindy Hui was the one who heard about ClotGuard from one of our posts on LinkedIn. She reached out to us to meet with someone from Microsoft to see how they can support our development. She wanted to help us secure labs and any other resources we may need. She connected us with Greg Carnie from Microsoft, who proposed the idea of having us develop our hardware with Microsoft.
Greg Carnie and Cody Church - Microsoft Both of them are the ones helping us with the collaboration with Microsoft to help us develop the patch/sensors for our product. They are looking to see to what extent Microsoft can help us (fabrication, design, etc.)
John Westworth - Microsoft John Westworth found out about ClotGuard recently, but has been championing a lot for us at Microsoft with this collaboration since he has seen a lot of our previous work. He is trying to get us whatever support we need from them as quickly as possible.
Azar Chatur - Director at The Knowledge Society (TKS) Azar Chatur was our director at TKS last year and helped us a lot throughout the summer and this year to secure opportunities to speak about ClotGuard and to pursue funding. He has been putting ClotGuard in the spotlight whenever we need support and is always looking for ways to help.
Brendan Samek - University of Alberta Brendan Samek is interested in what we are building at ClotGuard and wanted to support us by providing military connections to bypass the FDA process. He thought that our idea has a lot of potential in that specific market (he has worked with military-grade tools before) and also wanted to connect us to those in the wearables space. He has become an advisor, getting us connections to meet with those in our target markets.
Maleeka Malik - UCeed Maleeka Malik was our first contact with UCeed and connected us to multiple funds at UCeed. She was invested with what we are building and wanted to do whatever she could to get us access to some funding, and if not that, at least some support for UCeed in building our company.
Allison Swelin - UCeed Cenovus Allison Swelin was our UCeed Cenovus contact and championed ClotGuard and our support to the committee. She was invested in what we were building and was part of us securing the $5000 from UCeed Cenovus. Now, she is our advisor in residence helping us with the different challenges and needs of ClotGuard, and has already been instrumental is getting us the support and connections we need.
Partnerships/Collaborations/Funding
Making ClotGuard real also required finding a team of people who would be able to help us test all the components of ClotGuard, as well as help manage the business aspects. We've connected with 3 organizations that have been helping us develop the different aspects of ClotGuard.
University of Calgary
We've been working alongside Jeff Ryzner and Paula Berton, and the University of Calgary, to begin the proof of concept parts of testing for ClotGuard. Jeff Ryzner has been a champion for what we are developing at ClotGuard and connected us with Paula Berton so we can begin actual biochemsitry-related testing in the lab and make progress with validation. We've been in communication with Paula for the past few months to sort out the logistics of testing and plan out the first phases. The progress we've made so far with the University of Calgary looks like this:
- Had Paula conduct a literature review of the different components that ClotGuard utilizes and the advancements in those fields in the last 5 years
- Sent over our rough ClotGuard testing roadmap for Paula to review and provide feedback/changes on
- Mapped out the first phase of testing for ClotGuard, which is synthetic platelets development and protective coating tests
- Phases 1 and 2 (assessed together) would take roughly 24-30 months
- Need to meet to discuss budgeting
- Lab space
- Resources for testing
- Lab techs to run experiments
- Conduct an early patent landscape and FTO review
Microsoft
Our Microsoft collaboration was fostered through Cindy Hui and John Westworth, who introduced us to Greg Carnie and Cody Church, working at Microsoft, who help startups develop their prototypes and advance. Cindy reached out to us after seeing some of our work on ClotGuard and wanted us to connect with the people at Microsoft to see how they could support us. We have recently set up official communication with them and have made significant progress in developing our patch/sensor prototype components for ClotGuard. They have been helping us with the design and fabrication of our patch and sensors. The prototypes are either going to be shipped to us for testing from the Vancouver base, or they will be tested in house and have the results reported back to us. Our progress so far looks like this:
- Have sent over the requested materials to be used for the printing and development of the patch
- Set up a shared workspace for prototyping
- Have a rough outline of the patch exterior
- Have begun prototyping the internal components
- Microcontroller
- Cartridge
- Injector mechanisms
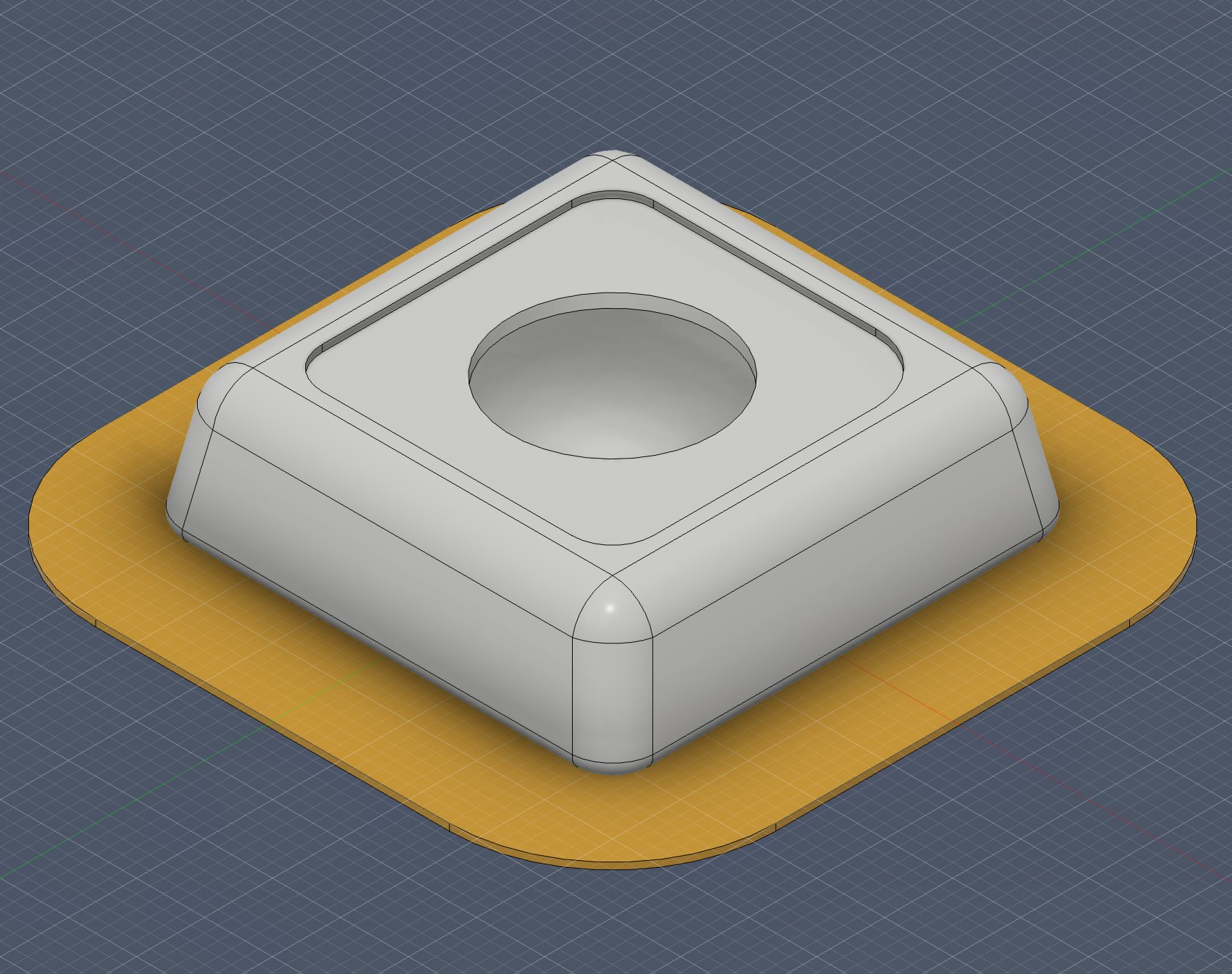 Patch exterior
Patch exterior
UCeed Cenovus Grant
We recently began our partnership with UCeed Cenovus to advance the development of ClotGuard. UCeed Cenovus is one of the grants from the University of Calgary that funds startups to continue building. We were awarded $5000 in non-dilutive funding and advisory support. We had originally met with Maleeka Malik to establish this partnership, and then, through her, met our main contact for UCeed Cenovus as well as our advisor, Allison Swelin. We had to present ClotGuard in front of the committee for the Cenovus grant. They were all very impressed with the amount of thought put behind the product, even though we didn't have any actual tests. They were also very enthusiastic about the potential of ClotGuard, and that is how we ended up gaining the funding and their support. We plan to use this funding to be put towards:
- Registering ClotGuard as a company in Alberta
- Lab space
- Lab resources
- Lab techs
- Website and design upgrades
- Promotions
We've already had our first advisory meeting to discuss registering the company as well as gain some more connections to the committee.
University of Alberta
Our very first partnership was with the University of Alberta through Michael Serpe, where we were at the very early stages of developing ClotGuard. We got to visit the university, tour Michael Serpe's lab and see the different innovations there. When we shared the info about ClotGuard, he was immediately enthusiastic about supporting us, even though we barely had any refined testing or validation. He and his lab were our first supporters. Now, being further into testing and development, we want to work with his lab for:
- Developing the patch's dissolvable microneedles
- Using PLGA materials for nanocarrier development
We've discussed different ways to carry out our testing with them, from having us go out to the university for testing, to having them at the lab develop and test, or potentially having them ship out the different components to Calgary for us to test.
Networking and Publicity Opportunities
Through the development of ClotGuard, in order to gain traction and validation, we also took the opportunity to present and talk about ClotGuard and different speaking engagements and networking events.
TKS Moonshot Presentations
Our first opportunity to present ClotGuard was where it was founded, in an innovation program called The Knowledge Society (TKS) Moonshot challenge. We presented in Calgary to a panel of judges and were able to secure first place in our cohort. This was the initial validation we got that ClotGuard seemed like a plausible idea.
IEEE Conference
In August, we had the opportunity to present ClotGuard at the IEEE Conference, a global conference that was being hosted in Calgary this year under their student founders program. At the event, we got to showcase the progress ClotGuard has made and secure many new connections who thought the idea was promising. This was also our first opportunity to present ClotGuard outside of a TKS event.
TKS Showcase
We presented ClotGuard at the mid-year TKS showcase, where TKS invites industry experts and startup mentors to view what the students are developing. Through this presentation, we earned new connections that were interested in supporting us and giving us more speaking engagement opportunities.
Conclusion
Next Steps
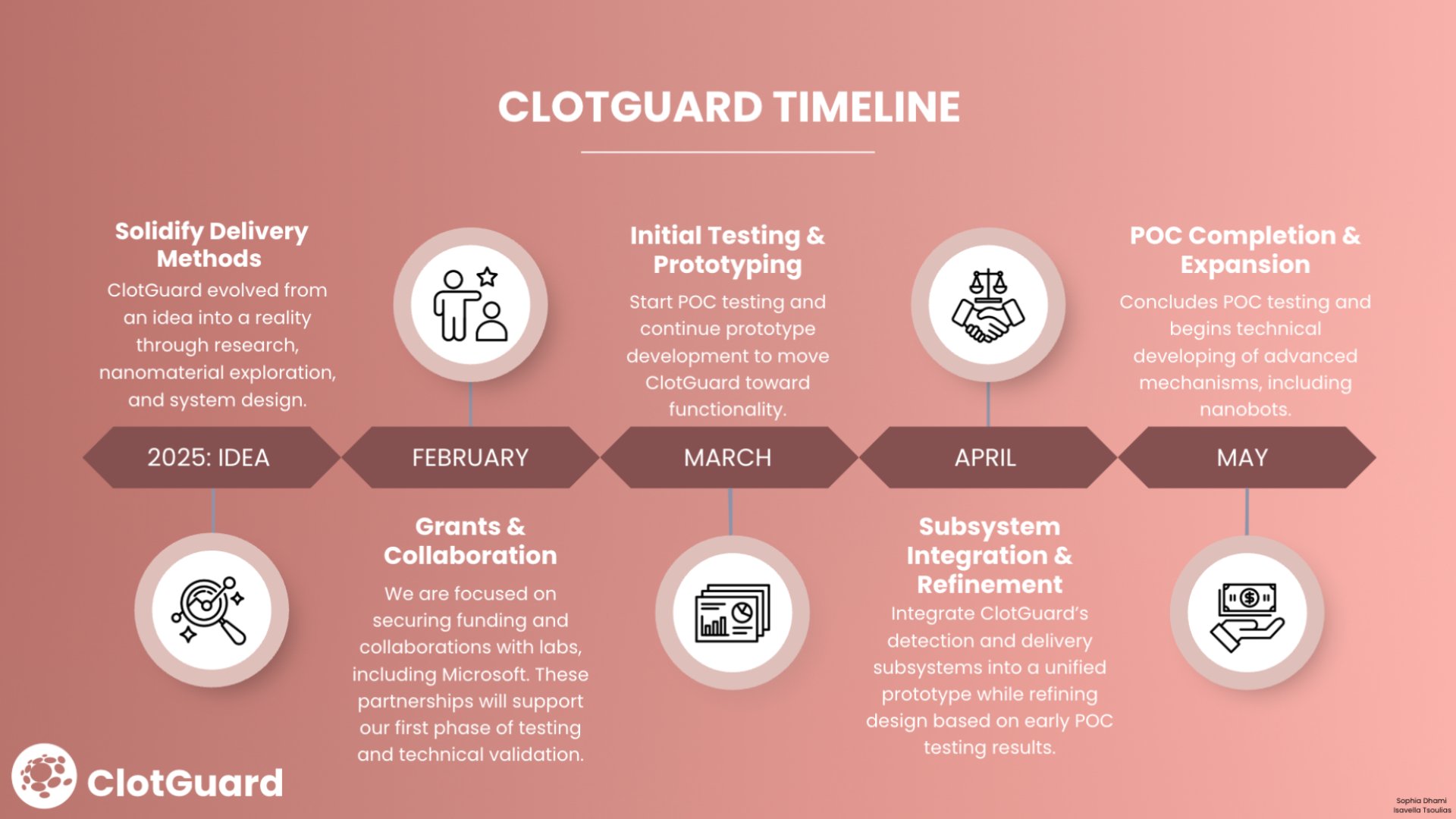
While we have done a lot of validation for ClotGuard and established a business case, we still need to conduct actual testing of these different components. Through current validation and research that we've done on our own and with the help of our advisors, we've found that:
- Utilizing synthetic lyophilized platelets to prevent hemorrhage is being researched and shows a lot of potential for being an effective treatment method
- Lyophilized platelets can last up to 3 years in storage while remaining stable
- Thrombin-cleavable peptides have been researched for enabling specificity in drug delivery
- Nanocarriers are being researched for different drug delivery applications and show promising results
- Tracking different biomarkers, such as heart rate, blood pressure, oxygen saturation, blood velocity, and shock index are all able to be tracked and are already in current medical devices and smartwatches
- Through our work with Microsoft, we have confirmed that we are able to create an injection mechanism that is triggered with biomarkers reaching a specific threshold
- PLGA is a safe bio-polymer to use in the construction of nanocarriers and will dissolve
- Linker molecules have been tested and approved for use in the body, and are effective in attaching a payload to a carrier (in this case, a platelet to a nanocarrier)
- Exposed collagen is an effective binding target as it is the earliest exposed protein when bleeding occurs, and can be found specifically where the tear of skin is located
- ClotGuard is a class 2 combination device, according to our advisor at the FDA
Applications of Technology
ClotGuard's end goal and primary use are for military applications in the medical space to treat the current problem of deaths on the battlefield due to hemorrhage. But, through more research and work with our advisors, we've begun considering and would want to eventually explore other applications such as
- Drug delivery
- Triggered delivery
- Hospital and emergency care situations
- First aid use
- Public use and protection
Citations
References
Alexandria, V. A. (2023, January 12). Federal Spending On Medical Supplies Tops $8.2 Billion. Health Industry Distributors Association. Retrieved February 15, 2026, from https://www.hida.org/hida/distribution/news/press-releases/2023/federal- spending-medical-supplies-8- billion.aspx#:\~:text=Federal%20Spending%20On%20Medical%20Supplies%20Tops%20$8.2%20Billion
Bertram, J. P., Williams, C. A., Robinson, R., Segal, S. S., Flynn, N. T., & Lavik, E. B. (2009, December 16). Synthetic Platelets: Nanotechnology to Halt Bleeding. Science Translational Medicine, 1(11). 10.1126/scitranslmed.3000397
Das, T., & Sultana, S. (2024, January 3). Multifaceted applications of micro/nanorobots in pharmaceutical drug delivery systems: a comprehensive review. Future Journal of Pharmaceutical Sciences, 10. https://link.springer.com/article/10.1186/s43094-023-00577-y
Eastridge, B. J., Hardin, M., Cantrell, J., Oetjen-Gerdes, L., Zubko, T., Mallak, C., Wade, C. E., Simmons, J., Mace, J., Mabry, R., Bolenbaucher, R., & Blackbourne, L. H. (2011, July). Died of wounds on the battlefield: causation and implications for improving combat casualty care. The Journal of Trauma, 71(1). 10.1097/TA.0b013e318221147b
Furman, M. I., Liu, L., Benoit, S. E., Becker, R. C., Barnard, M. R., & Michelson, A. D. (1998, March 17). The cleaved peptide of the thrombin receptor is a strongplatelet agonist. The National Academy of Sciences, 95, 3082-3087. https://doi.org/10.1073/pnas.95.6.3082
Gupta, A., Soni, S., Chauchan, N., Khanuja, M., & Jain, U. (2022, September). Nanobots-based advancement in targeted drug delivery and imaging: An update. Journal of Controlled Release, 349, 97-108. https://doi.org/10.1016/j.jconrel.2022.06.020
Hu, M., Ge, X., Chen, X., Mao, W., Qian, X., & Yuan, W.-E. (2020, July 15). Micro/Nanorobot: A Promising Targeted Drug Delivery System. Pharmaceutics, 12(7). 10.3390/pharmaceutics12070665
Katzenell, U., Ash, N., & Tapia, A. L. (2012, September). Analysis of the Causes of Death of Casualties in Field Military Setting. Military Medicine, 177(9). 10.7205/MILMED-D-12-00161
Khan, Z., Khan, N., Geetha, M., Veettil, R. P., Kasote, D. M., Hasan, A., & Sadasivuni, K. K. (2025, June 4). Therapeutic applications of nanobots and nanocarriers in cancer treatment. Analytical Science, 41, 1305-1324. https://link.springer.com/article/10.1007/s44211-025-00799-5
Ko, P.-T., Lee, I.-C., Chen, M.-C., & Tsai, S.-W. (2015, June). Polymer microneedles fabricated from PCL and PCL/PEG blends for transdermal delivery of hydrophilic compounds. Journal of the Taiwan Institute of Chemical Engineers, 51, 1-8. https://doi.org/10.1016/j.jtice.2015.01.003
Kong, X., Gao, P., Wang, J., Fang, Y., & Hwang, K. C. (2023, July 14). Advances of medical nanorobots for future cancer treatments. Journal of Hematology and Oncology, 16. https://link.springer.com/article/10.1186/s13045-023-01463-z
Kuhn, B. J., Swanson, A., Cherupalla, A. S., Booth, L., Dickerson, W. M., Fitzpatrick, G. M., Alexander, W. A., & Moskowitz, K. A. (2024, March). Mechanisms of action of an investigational new freeze-dried platelet-derived hemostatic product. Journal of Thrombosis and Haemostasis, 22(3), 686-699. https://doi.org/10.1016/j.jtha.2023.11.022
Latif, R. K., Clifford, S. P., Baker, J. A., Lenhardt, R., Haq, M. Z., Huang, J., Farah, I., & Businger, J. R. (2023, May 24). Traumatic hemorrhage and chain of survival. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 31(25). 10.1186/s13049-023-01088-8
Lee, J. W., Park, J.-H., & Prausnitz, M. R. (2008, February 7). Dissolving Microneedles for Transdermal Drug Delivery. Biomaterials, 29(13), 2113-2124. 10.1016/j.biomaterials.2007.12.048
National Heart, Lung, and Blood Institute. (2024, July 2). A potential game-changer for emergency medicine: synthetic platelets. NHLBI.NIH.gov. Retrieved February 28, 2026, from https://www.nhlbi.nih.gov/news/2024/potential-game-changer- emergency-medicine-synthetic-platelets
National Institute for Health and Care Research. (2022, June 28). Improving outcomes after trauma and blood loss. National Institute for Health and Care Research. Retrieved February 15, 2026, from https://www.nihr.ac.uk/story/improving-outcomes- after-trauma-and-blood-loss
National Institutes of Health. (2024, April 30). Synthetic platelets stop bleeding in animal studies. National Institutes of Health. Retrieved February 28, 2026, from https://www.nih.gov/news-events/nih-research-matters/synthetic-platelets-stop-bleeding- animal-studies
Ohanian, M., Cancelas, J. A., Davenport, R., Pullarkat, V., Hervig, T., Broome, C., Marek, K., Kelly, M., Gul, Z., Rugg, N., Nestheide, S., Kinne, B., Szczepiorkowski, Z., Kantarjian, H., Pehta, J., Biehl, R., Yu, A., Aung, F., Antebi, B., & Fitzpatrick, G. M. (2022, March 1). Freeze-dried platelets are a promising alternative in bleeding thrombocytopenic patients with hematological malignancies. American Journal of Hematology, 97(3), 256-266. 10.1002/ajh.26403
Ontario Association of Paramedic Chiefs. (2021, May 25). Be Citizen Ready: Control the Bleed – Paramedic Services Week 2021 Blog Series. Ontario Association of Paramedic Chiefs. Retrieved February 15, 2026, from https://www.oapc.ca/citizen- ready-control-bleed-paramedic-services-week-2021-blog-series/
Periayah, M. H., Halim, A. S., & Saad, A. Z. M. (2017, October 1). Mechanism Action of Platelets and Crucial Blood Coagulation Pathways in Hemostasis. International Journal of Hematology-Oncology and Stem Cell Research, 11(4), 319-327. https://pmc.ncbi.nlm.nih.gov/articles/PMC5767294/
Sartawi, Z., Blackshields, C., & Faisal, W. (2022, August). Dissolving microneedles: Applications and growing therapeutic potential. Journal of Controlled Release, 248, 186-205. https://doi.org/10.1016/j.jconrel.2022.05.045
Sum, R., Hager, S., Pietramaggiori, G., Orgill, D. P., Dee, J., Rudolph, A., Orser, C., Fitzpatrick, G. M., & Ho, D. (2007, April). Wound-healing properties of trehalose-stabilized freeze-dried outdated platelets. Transfusion, 47(4). 10.1111/j.1537- 2995.2007.01170.x
Trivedi, A., Potter, D. R., Miyazawa, B. Y., Lin, M., Vivona, L. R., Khakoo, M. A., Antebi, B., Lee, A., Holcomb, J. B., Fitzpatrick, G. M., & Pati, S. (2021, February 1). Freeze-dried platelets promote clot formation, attenuate endothelial cell permeability, and decrease pulmonary vascular leak in a murine model of hemorrhagic shock. Journal of Trauma and Acute Care Surgery, 90(2), 203-214. 10.1097/TA.0000000000002984
Tsoulias, I., & Dhami, S. (2025, May 1). ClotGuard: Integrating Nanobots and Biosensors to Redefine Hemostasis [Article]. Medium. Retrieved February 17, 2026, from https://medium.com/@IsavellaT/tiny-bots-big-impact-revolutionizing-healing- with-platelet-nanobots-4ebeef6d8ebc
Wang, Y., Wu, H., Zhou, Z., Maitz, M. F., Liu, K., Zhang, B., Yang, L., Luo, R., & Wang, Y. (2022, March 4). A thrombin-triggered self-regulating anticoagulant strategy combined with anti-inflammatory capacity for blood-contacting implants. Science Advances, 8(9). 10.1126/sciadv.abm3378
Wolkers, W. F., Walker, N. J., Tablin, F., & Crowe, J. H. (2001, March). Human platelets loaded with trehalose survive freeze- drying. Cryobiology, 42(2), 79-87. 10.1006/cryo.2001.2306
Wolkers, W. F., Walker, N. J., Tamari, Y., Tablin, F., & Crowe, J. (2002, September). Towards a Clinical Application of Freeze- Dried Human Platelets. Cell Preservation Technology, 1(3), 175-188. 10.1089/153834402765035617
Yang, J., Zeng, H., Luo, Y., Chen, Y., Wang, M., Wu, C., & Hu, P. (2024, September 14). Recent Applications of PLGA in Drug Delivery Systems. Polymers, 16(18). https://pmc.ncbi.nlm.nih.gov/articles/PMC11435547/
Zhang, X., Yin, Z., Xiang, S., Yan, H., & Tian, H. (2024, October 3). Degradation of Polymer Materials in the Environment and Its Impact on the Health of Experimental Animals: A Review. Polymers, 16(19). 10.3390/polym16192807
Zhao, L., Sabri, A. H. B., McGuckin, M. B., Li, L., Wang, Z., Larrañeta, E., & Donnelly, R. F. (2024, October 23). Implantable Microarray Patch: Engineering at the Nano and Macro Scale for Sustained Therapeutic Release via Synthetic Biodegradable Polymers. Advanced Materials Technologies, 10(6). https://doi.org/10.1002/admt.202400346
Acknowledgement
- Sophia Dhami - Co-Founder of ClotGuard: Sophia Dhami is my active co-founder on ClotGuard. Everything detailed in here has been developed alongside her with equal contribution. I am showcasing the work that we have developed together and acknowledge that it is our idea, and I get the opportunity to participate in experiences like this within school, unlike her.
- Michael Serpe - University of Alberta at Gunning/Lemieux Chemistry Centre: Got the opportunity to tour the Gunning/Lemieux Chemistry Centre, led by Michael Serpe, who was very interested in what we were developing at ClotGuard, as well as our earliest validator/supporter. We specifically reached out to discuss the dissolvable microneedle and PLGA nanoparticle technologies he was developing in his lab. We established having him as an advisor as well as a future collaborator once we begin active testing.
- Ejaife Agbani - University of Calgary: Met with Ejaife Agbani to discuss the hemostasis and platelet components of ClotGuard. He gave us some guidance on how to proceed with future testing (like different literature reviews and papers to read).
- Sara Akbarzadeh - Medical Wearables Reviewer at the FDA: Sara met with us to review the theoretical idea for ClotGuard and gave us an overview of the FDA approval process for a device like ours (labelled a combination device). She validated our idea from an FDA perspective, and she also gave us a rough timeline and asked us to stay updated with our progress.
- Noah Smith - IP Analyst at Front Row Ventures: Gave him an overview of the idea for ClotGuard and discussed what IP would look like in the future. He gave us a roadmap for the IP process and when we should begin it. We also discussed future collaboration with Front Row Ventures once we are eligible (of age) for funding.
- Jeff Ryzner - University of Calgary at the Hunter Hub for Entrepreneurial Thinking: Met with Jeff Ryzner to discuss lab opportunities to begin the testing portion for ClotGuard. He was extremely excited about working with us and was determined to help us in any way possible. He connected us to Paula Berton, who would guide us through the actual testing process. He is an advisor for ClotGuard and is able to get us future connections/resources.
- Paula Berton - University of Calgary: Paula Berton is our connection at the University of Calgary, who can help us in the direct testing process by guiding us on our testing roadmap, delegating and planning the different phases of testing and the components/protocols, as well as helping us secure resources like lab space, funding, and support for testing.
- Pablo Guzman - Material Science at A&M Texas: Pablo Guzman is helping us with validating the material science components of ClotGuard, as well as helping us with some of the design of the different mechanisms we are using, such as the storage/delivery methods. He validated ClotGuard and said that the process makes sense and logically works, and he asked to keep getting updates from us as we progress.
- Alexandra Ramadan - X, The Moonshot Factory: Alexandra Ramadan first helped us with ClotGuard when she judged our project at the TKS Moonshots Presentations, where she gave a lot of good feedback about our idea and found it very interesting. Recently, we connected with her again to update her on what we’re working on for ClotGuard and some of the support we’re looking for. She asked us to keep her updated and also send over some of the labs we are looking to work on so she can see if anything would work for us. She validated our idea, especially how much it had progressed since the initial judging she did for it.
- Cindy Hui - AtlaML: Cindy Hui was the one who heard about ClotGuard from one of our posts on LinkedIn. She reached out to us to meet with someone from Microsoft to see how they can support our development. She wanted to help us secure labs and any other resources we may need. She connected us with Greg Carnie from Microsoft, who proposed the idea of having us develop our hardware with Microsoft.
- Greg Carnie + Cody Church - Microsoft: Both of them are the ones helping us with the collaboration with Microsoft to help us develop the patch/sensors for our product. They are looking to see to what extent Microsoft can help us (fabrication, design, etc.)
- John Westworth - Microsoft: John Westworth found out about ClotGuard recently, but has been championing a lot for us at Microsoft with this collaboration since he has seen a lot of our previous work. He is trying to get us whatever support we need from them as quickly as possible.
- Azar Chatur - Director at The Knowledge Society (TKS): Azar Chatur was our director at TKS last year, and helped us a lot throughout the summer and this year to get different opportunities to speak about ClotGuard and get funding opportunities. He has been putting ClotGuard in the spotlight whenever we need the support and is always looking to see how he can help.
- Maleeka Malik - Was our contact for funding from UCeed and connected us with the different funds at the university. Championed our work to the committee to ultimately have us secure funding.
- Allison Swelin - Was our contact for the UCeed Cenovus grant, and was very impressed with what we were building and our drive to build this. Championed our work to the Cenovus committee and was keen on getting us funding. She is also our main point of contact for UCeed advisory support and is helping us with some of the challenges with ClotGuard.
- UCeed Cenovus - The organization and committee that awarded us the $5000 funding and is currently offering us support.
- Arissai Filleul - Early ClotGuard creator: Arissai Filleul was a part of the very early development of ClotGuard, but chose not continue with us after a couple of months of development.
- ChatGPT: Used for a lot of the ideation and brainstorming of ClotGuard and potential technological components to include when coming up with the idea presented here.
- Google: Where we found a lot of the research and papers that justified our technical components and business case.