
How/which stem cells, multi-potent vs. pluripotent, are viable treatments for Alzheimers Disease
Shreya Kaushik
Master's College
Grade 11
Presentation
No video provided
Problem
Alzheimer's is the most popular form of dementia, and estimates say this disease is set to nearly double in occurrence by 2050. Late onset Alzheimer's typically affects our old age community, 65 and above, but early onset Alzheimer's can affect younger individuals as well. Exciting and new research suggests that stem cells may have positive effects on Alzheimer's. Abucanumab, N-methyl-D-aspartate blocker, and a few other drugs have been approved by the United States Food and Drug Administration but are only able to relieve AD symptoms temporarily. Currently all treatments and medications focus on associated symptoms of AD but fail to solve the root of the problem, therefore there is no “cure” for Alzheimer's Disease.
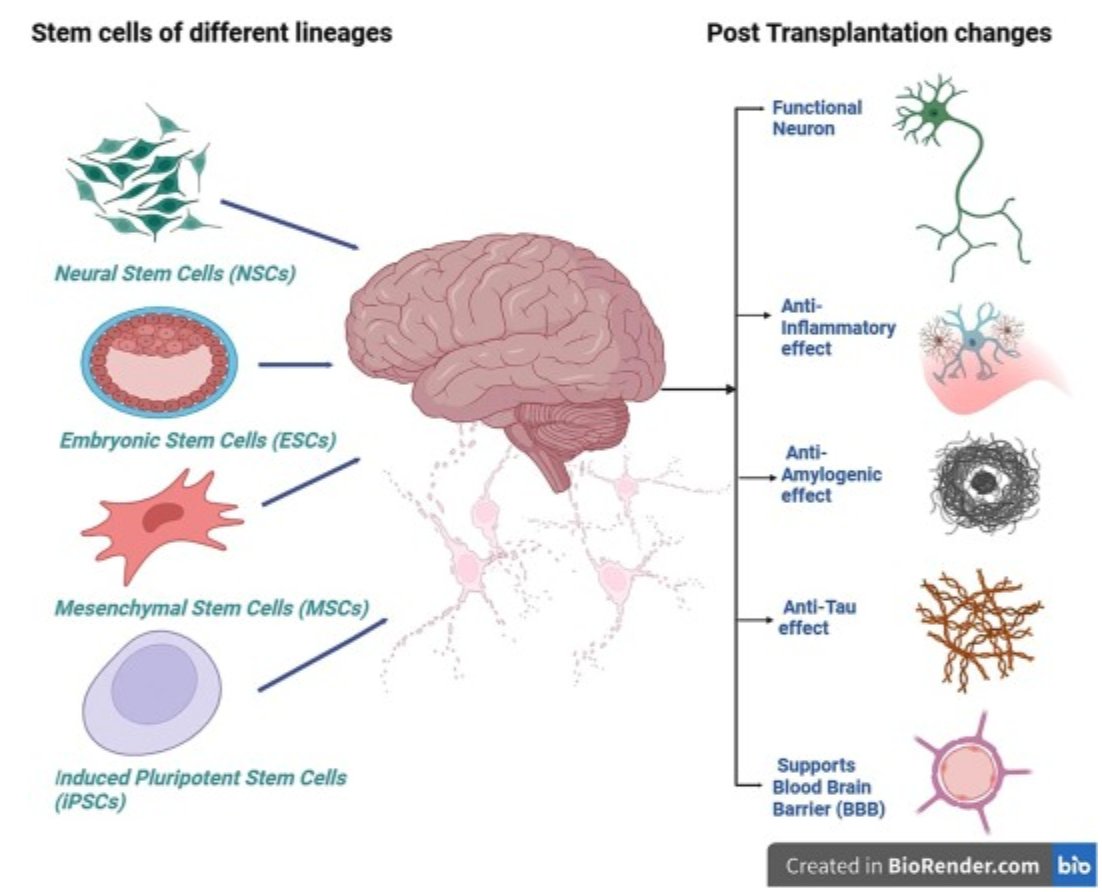
The discovery of stem cells dates back to the 1963s when Drs. James Till and Ernest McCulloch looked into bone marrow for blood cell maturation research. They found stem cells within the bone marrow. Stem cells are unspecialized cells that have the ability to self-renew indefinitely and can specialize themselves into specific cells, making them necessary for tissues and repair. There are two specific subsections of stem cells, embryonic which are pluripotent (can become anything) and adult stem cells which are multipotent (are limited). As well, with evolving technology, scientists are able to make Induced Pluripotent Stem Cells, iPSCs, in labs. Stem cells, specifically Neural Stem Cells (NCS), Embryonic Stem Cells (ECS), Induced Pluripotent Stem Cells (iPSC) and Mesenchymal Stem Cells (MSCs), may be able to regenerate neural networks and improve cognitive function, ultimately serving as a cure for Alzheimer's disease. This research paper will cover the structure and function of stem cells, looking into their unique differentiation and self-renewable abilities and how they will become a treatment for neurological diseases such as Alzheimer's. Furthermore, this paper will deep dive into the disruptions within the neurological system of a brain with Alzheimer's and how stem cells will replace and renew aspects of the neurological system that are directly related to Alzheimer's, both pathological and pathophysiological.
Method
Overview of Alzheimer's Disease:
- General knowledge about Alzheimer's
- Pathology of Alzheimer's
- Amyloid plaques and Tau
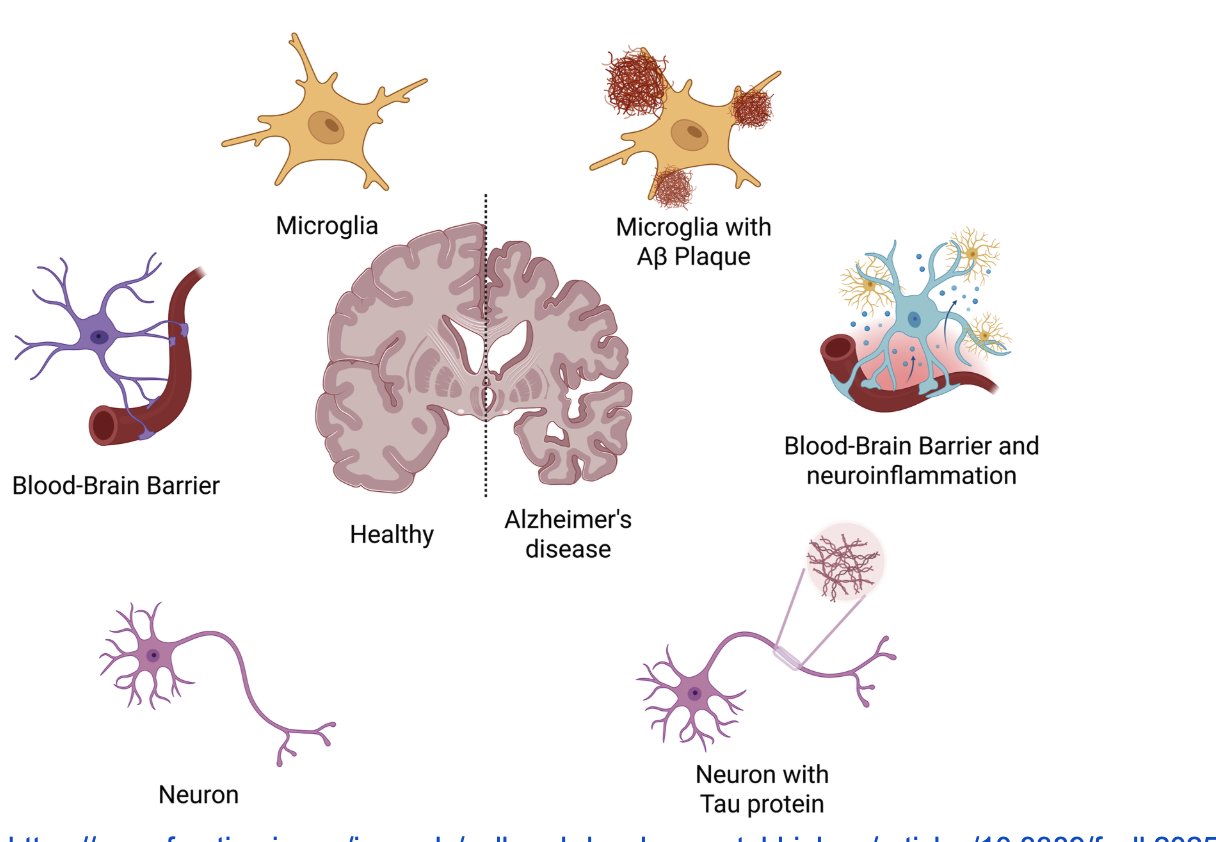
Amyloid plaques and tau tangles are the two misfolded proteins within the brain that are direct pathological causes of Alzheimer's disease and are causes of further deterioration of the brain.
- Pathophysiological Causes of Alzheimer’s
- Neuroinflammation
- Mitochondrial Damage
- Neural Cholesterol Levels and Fatty Acid Metabolism
This includes neuroinflammation, mitochondrial damage, neural cholesterol levels and fatty acid metabolism which are recognized associated pathophysiological causes of Alzheimer's.
Analyzing Stem Cells:
- Multipotent vs Pluripotent
The differences between multipotent and pluripotent stem cells, such as differentiation and self-renewable capabilities and inherent limitations as a treatment.
Types of Stem Cells for potential Alzheimer's treatment
- Neural stem cells (NSCs)
- Embryonic stem cells (ESCs)
- Mesenchymal Stem Cells (MSCs)
- Induced Pluripotent Stem Cells (iPSCs)
How each type of stem cell has been specifically tested and researched to determine the best option for Alzheimer's.
- Clinical Trials
The clinical trials that have been performed and how these results describe the feasibility of stem cells as treatment.
Research
ALZHEIMER'S DISEASE
Alzheimer's disease can be categorized into 3 overarching stages or phases, those being early, mid, and late. Early stage Alzheimer's is mild and allows the patient to still function normally, however they do begin to start losing memories and bits of information. Overall, it is hard to notice symptoms at this stage but if diagnosed early, the patient has the best chance at slowing the rate of brain deterioration. The middle stage is typically the lengthiest and can last for up to years. The brain continues to deteriorate slowly and the patient will need increased assistance and care. The nerves within the brain become more damaged but they will still have some minimal awareness. Late stage Alzheimer's is severe and irreparable. The patient begins to lose cognitive abilities and significant personality changes can be seen. They also are unable to communicate verbally therefore the patient will need major and continuous assistance and often will be in caregiving facilities at this point.
Overall Alzheimer's is specified into 7 exact stages based on Global Deterioration Scale (GDS).
| Stage | Symptoms |
|---|---|
| Stage 1 |
|
| Stage 2 |
|
| Stage 3 |
|
| Stage 4 |
|
| Stage 5 |
|
| Stage 6 |
|
| Stage 7 |
|
This graph is provided from the source OVERVIEW. (n.d.). Alzheimer Society. Retrieved March 3, 2026, from https://alzheimer.ca/sites/default/files/documents/Progression-Overview-Alzheimer-Society.pdf https://alzheimer.ca/sites/default/files/documents/Progression-Overview-Alzheimer-Society.pdf
PATHOLOGY OF ALZHEIMER'S DISEASE
Two of the main contributing proteins to the result of Alzheimer's Disease are misfolded amyloid or Aβ and tau.
The pathological criteria for Alzheimer's Disease states that the formation is of extracellular Aβ plaques and intracellular tau accumulation. The amyloid is abnormal protein fibers that clump together in tissues, causing damage and leading to diseases called amyloidoses, which includes Alzheimer's. When healthy proteins unravel and aggregate, interfering with cellular processes leads to degeneration. APP or Amyloid Precursor Protein is misfolded and unstable and is spliced by beta-secretase and then gamma-secretase after translation during protein synthesis. Through this splicing, APP is turned into the protein Amyloid Beta (or Aβ). Aβ continues to build up in the brain, causing amyloid plaques, leading to neurodegenerativeness. This is known as the Amyloid Cascade Hypothesis as it leads to neurological damage, tau tangles and cell death. Unfortunately, the Amyloid Cascade Hypothesis has been challenged as it does not provide an explanation for the silent period or preclinical stage. The silent period can last for up to 20 years before any noticeable AD symptoms appear. The noticeable silent period of Alzheimer's disease occurs before there are any visible symptoms of the disease, therefore before the traditional “early” stage of AD. Amyloid plaques and tau tangles begin to be observed as the brain slowly starts to shift. Hence, why they are recognized as the main pathological contributors to Alzheimer's. It is difficult to intervene or find the silent period of the brain and it can only be done through research such as PET scans or spinal fluid biomarkers.
The tau protein is crucial for maintaining microtubal stability, which is the cell's internal transportation system. In the case of AD, tau becomes hyperphosphorylated causing the microtubules to disassemble and the tau aggregates into paired helical fragments. These tau tangles or neurofibrillary tangles are tau protein build up as more and more tau becomes hyperphosphorylated and detached.
Clinical trials show results for regulators of Aβ and tau under the form of straightforward amyloid and tau immunotherapy as negative, suggesting that the real cause for AD may be different. Because of this, we know that inhibiting Aβ and tau as AD treatment is not an option and therefore we need an alternative treatment.
Other theories include the Vascular Hypothesis, which states that AD is related to blood vessels within the brain largely with the reduction of blood flow. It combines neurological dysfunction such as AD and cardiological diseases. Breakdown of the blood-brain barrier (BBB) results in neurotoxic serum protein accumulation and synaptic dysfunction are all related causes of the Vascular Hypothesis. This creates a cycle of amyloid beta cells buildup and pathology.
PATHOPHYSIOLOGICAL CAUSES FOR ALZHEIMER'S DISEASE
Though the pathophysiology of AD is still largely a mystery, neuroinflammation, abnormal microglia activation, metabolic failure, oxidative stress, and sustained cholesterol-associated neuronal distress are all known and potential targets for intervention.
Based on the relations between old age and AD, inflammation within the brain is likely a cause. Neuroinflammation is technically the Central Nervous Systems natural immune response to infections and toxins. Glial cells (specifically microglia and reactive astrocytes) are activated and release inflammatory mediators, which is normally used to protect the brain from infections and autoimmune attacks but is also a driver for Alzheimer's disease. Abnormal microglia activation means microglia will activate and react to pathogens but then are “stuck” in the activation phase. They continuously release neurotoxic factors that begin to attack healthy neurons and brain tissue, therefore becoming chronic. Chronic or excessive inflammation can damage neurons, serving as a direct contributor to neurodegeneration. Animal models and clinical trials are focusing on blocking or enhancing inflammatory pathways in the Central Nervous System. However there are still many complex variables that contribute to neuroinflammation.
Damaged mitochondria accumulation as well as may be a cause for age-related neurodegenerative diseases. This is called Mitochondrial Dysfunction where there can be mutations within mitochondrial DNA and dysfunction of mitochondrial axonal transport. Effects of mitochondrial DNA play roles in pathogenesis which can result in ATP depletion, oxidative stress and synaptic dysfunction. Building on this research, I know that mitochondrial DNA is directly inherited from the maternal side of an individual's family. Therefore, mtDNA mutations and dysfunction should theoretically be tracked and directly linked to the individual's mother and maternal family. If the individual's mother suffers from mtDNA mutations or mitochondrial axonal transport dysfunctions, it is highly likely the offspring will inherit these dysfunctions. Statistics show that 1 to 2% of Alzheimer's cases are inherited in an autosomal dominant manner and are presymptomatic (genetically predisposed to developing Alzheimer's Disease) but I believe there could also be a linkage to AD maternally through Mitochondrial Dysfunction. Other Alzheimer's cases are believed to be asymptomatic, they have amyloid buildup within the brain but lack cognitive symptoms. Some of these individuals may never progress to clinical Alzheimer's, or it would take over 20 years.
Lastly, abnormalities in neuronal cholesterol levels and fatty acid metabolism likely contribute to AD. Cholesterol is a type of lipid, which is three conjoined fatty acid chains on a glycerol backbone. Cholesterol is needed to build cells, makes certain hormones and Vitamin D. Cholesterol 24-hydroxylase and cholesterol 27-hydroxylase are cytochrome P450 enzymes that produce important oxysterols (CYP46A1 and CYP27A1) through oxidation. Immunocytochemical studies show that these oxysterols are expressed in neurons and some astrocytes in the normal brain. In Alzheimer's Disease CYP46A1 shows expression in astrocytes and amyloid plaques but CYP27A1 decreases in neurons altogether. Overall these oxysterols are important for brain cholesterol regulation, the blood-brain barrier (BBB) and neurotransmission.
STEM CELLS
Stem cells are unspecialized cells that have the ability to self-renew and differentiate into the necessary cells, usually for organ or tissue development. When cued to do so, stem cells specialize. Stem cells can be found in multiple different areas of the human body and typically named after the place of origin. They have certain characteristics that make each type of stem cell different from the others. Typically during mitosis, stem cells will split to produce one daughter cell that is specialized and the other would be another stem cell, and therefore unspecialized.
For neurological diseases, researchers use various stem cells like Mesenchymal Stem Cells (MSCs) from bone marrow/fat, Neural Stem Cells (NSCs), Induced Pluripotent Stem Cells (iPSCs), and sometimes Embryonic Stem Cells (ESCs). I will be overviewing these four specific stem cells in my research to determine the best possible treatment therapy.
MULTIPOTENT VS PLURIPOTENT STEM CELLS
There are two types of stem cells found within the body, multipotent or pluripotent. Understanding the difference between these stem cells is an integral part of understanding treatment methods and options.
Multipotent stem cells are adult stem cells that have the capabilities to self-renew or differentiate into different cells. Neural Stem Cells and Mesenchymal Stem Cells are common examples of these. These cells are typically smaller in number and only begin to specialize when they perceive signals to do so, such as repairing tissue or organ damage of particular parts. Furthermore, since these cells are already adults, they are limited in terms of types of cells that they can differentiate into. These stem cells can provide more centralized and specific therapies for diseases.
Pluriopotent stem cells are the more well known and “true” stem cells. They are able to differentiate themselves into any type of cell within the human body. Examples include Embryonic Stem Cells and Induced Pluripotent Stem Cells (though these are technically adult stem cells, they are programmed to behave like embryonic stem cells.). Pluripotent cells therefore are able to be used as treatment for multiple body parts and systems since they have the flexibility to specialize into any type of cell that originated from the 3 embryonic germ layers, the Endoderm, Mesoderm and Ectoderm.
NEURAL STEM CELLS
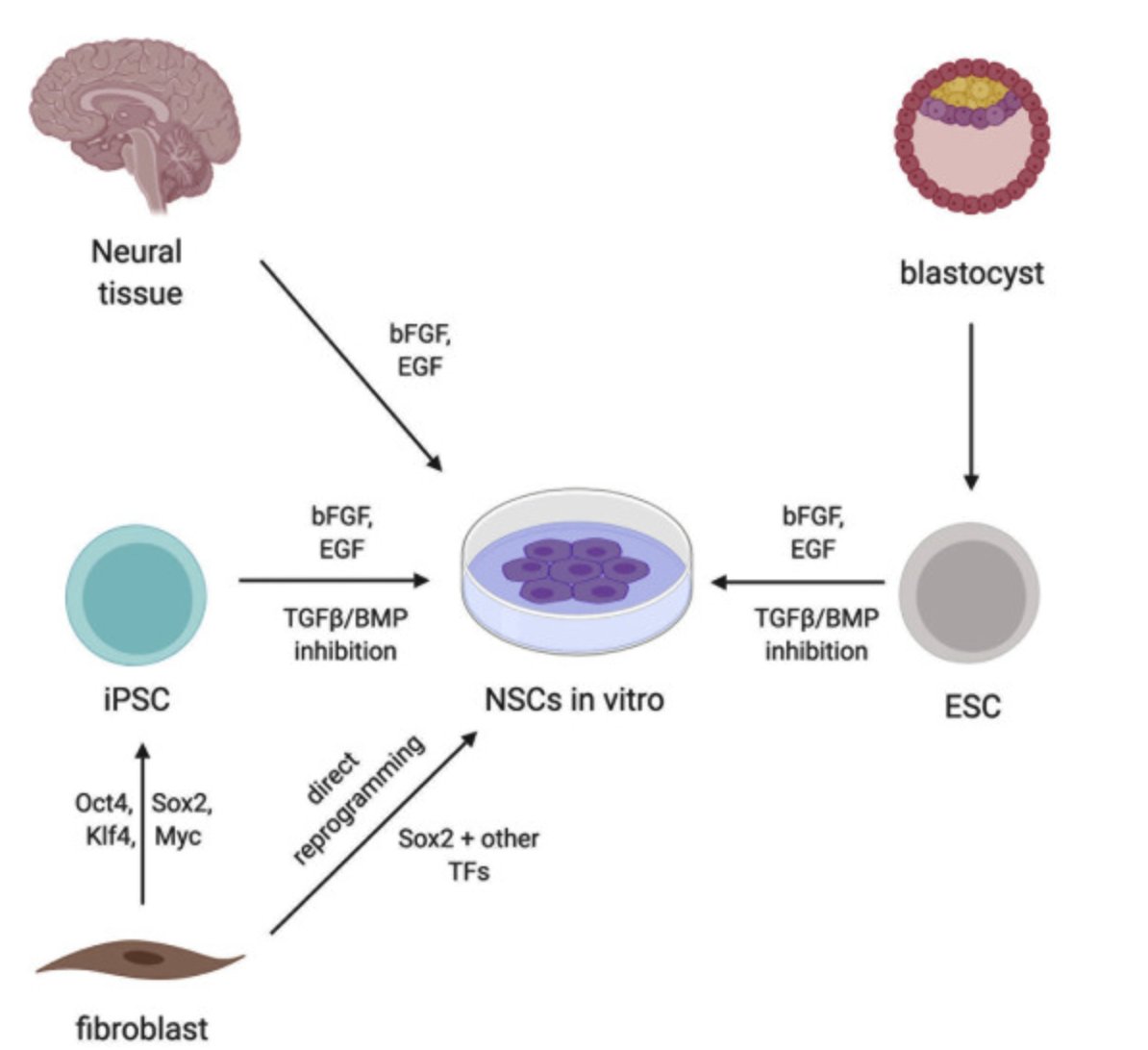
Neural stem cells (NSC) are stem cells of the nervous system and are formed during fetal development. In an adult brain, there is a very limited amount of NSC’s which are mainly dormant but there is some evidence proving that NSC’s have direct implications/ roles on brain plasticity, disease, aging and regeneration. The limited number of NSC’s within the nervous system is the main restricting factor for NSC therapies and clinical applications. The behaviors of different types of stem cells are strongly influenced by their location, therefore their “stem cell niche.” Their niches provide ample nutrients, regulation and maintenance and physical support for these stem cells.
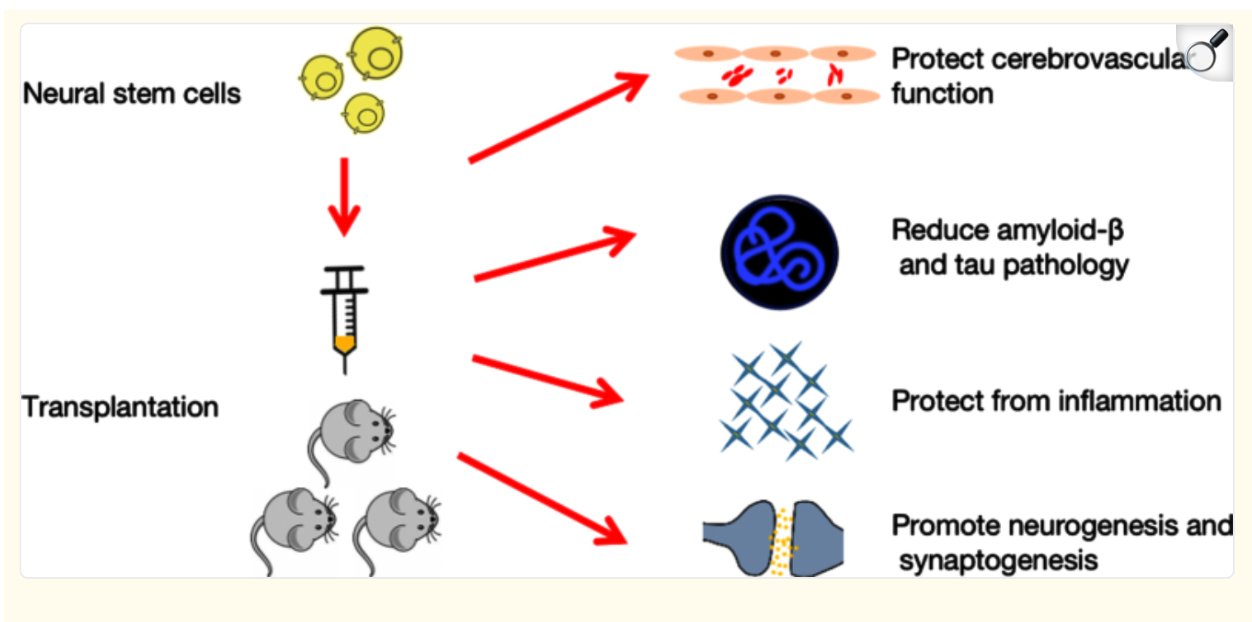
NSCs are multipotent stem cells that are typically found in the developing and central nervous system of most mammals. They usually differentiate into neurons, astrocytes, and oligodendrocytes within the nervous system. For stem cell therapy, specifically in the case of Alzheimer's Disease, they function through two main processes or mechanisms. The first group manages the damaged neurons within the brain and restores them. The second group controls brain synapsis by secreting many neurotropic factors which are mediated via paracrine actions.
Some issues are also foreseeable with the use of mouse models to reflect human AD. There are many limitations and arguments that they are not yet fully able to model humans with Alzheimer's Disease. Mainly related to the late onset of pathology, diverse genetic backgrounds, gender disparities in pathology and significant variability in Aβ levels during tests. Therefore it is difficult to exactly determine benefits of NSC transplants and it is important that transgenic murine mice models are used to overcome many of these problems. Typically NSCs are transplanted into the hippocampus of the model and after one to six months. Then researchers will start tracking the efficiencies of NSC transplantation on the mice.
An amyloid precursor protein mouse model was created by planting human-derived neural stem cells AKA hNSCs. When this was tested, hNSCs cured learning, memory and identification but not anxiety in mice with AD. As well, Aβ plagues did not particularly decrease but the densities of synapsis, neurons and neurofibrils in the hippocampus and frontal cortex of the brain increased. Spatial memory and learning was also enhanced. l-Shin Lee used the help of the rat neuron-specific enolase (NSE) promoter on mutant mice with APP to study the therapeutic effects of fetal human NSCs. They found that some of the stem cells were able to differentiate into neurons or glial cells and improved spatial memory of the mice. There was also a reduction in tau and Aβ through signalling reduction of BACE1 (beta-site amyloid precursor protein), therefore inhibiting Aβ and tau secretions. It further controlled the secretion of inflammatory mediators through microglia-mediated inactivation or anti-inflammatory secretion and improved synaptic brain plasticity overall.
The main drawbacks and risks of neural stem cell therapy, along with ethics, consists of immune rejection, genetic mutations, and the potential for tumorigenesis. Tumors would likely occur from the uncontrolled proliferation of NSCs in the brain after administering transplantation. Cell source and dosage, mode of transplantation and timing are important factors to consider as well.
EMBRYONIC STEM CELLS
Naturally, ESCs are usually found in the placenta but now can be grown through in vitro and are still able to differentiate into the 3 germ layers, the Endoderm, Mesoderm and Ectoderm. Specifically, ESCs can differentiate into basal forebrain cholinergic neurons or BFCNs. One particular test transplanted BFCNs from mice and ESCs from humans into the basal forebrain of mice modelling AD. They found positive results from this test where the BFCNs progenitors developed into mature cholinergic neurons. These neurons then helped with cognitive impairment that is an associated symptom of Alzheimer’s Disease. Scientist Yan Liu differentiated human ESCs (hESCs) into an almost homogenous group of NKX2.1 MGE-like progenitor cells. These specific cells gave rise to GABA interneurons, which are important for many cognitive and neural functions, and more BFCNs. These BFCNs connect to hippocampal neurons, in turn helping with learning and memory.
Although there is a lot of evidence supporting ESC, there are some inherent risks to this form of therapy. There is trouble with accessibility, which is limited by immunogenic rejection, unregulated cell proliferation and cancer-causing potential from the over stimulation of cell growth. ESC’s typically have to be derived from the blastocyst, posing a huge ethical issue since a possible embryo is being destroyed. As well since ESCs often lead to immune rejection and graft-versus-host disease once implanted, often the patient has to take immunosuppressive drugs after implantations. ESCs are continuing to be used to create animal research models for diseases such as Alzheimer's.
MESECHYMAL STEM CELLS
Mesenchymal Stem Cells are found in various parts of the human body, but most typically in bone marrow. They are adult stem cells and they typically differentiate into mesodermal cells. Of which includes adipocytes, chondrocytes, and osteoblasts. MSCs and neural cells may interact but usually through some sort of bystander cell. MSCs have the ability to help with AD by providing a neuroprotective milieu and they do this by exerting anti-inflammatory and antiproliferative effects on microglia and astrocytes. As well, MSCs have the ability to stimulate the growth of localized neural precursor cells, and therefore allow them to grow into adult cells.
MSC’s have also had successful preclinical trials as a treatment for Alzheimer's Disease. Mice were given hMSC intravenous injections and these tests tell us that hMSCs have amyloid-degrading and anti-inflammatory properties, which we know are major contributors to AD. After one week, a single injection of hMSC had enormous effects on reducing soluble Aβ levels. After ten weeks, there was a significant reduction of Aβ plagues and neuroinflammation. As well, stem-cell exosomes, tiny vesicles that work as messengers for intracellular processes, are also being researched. BMSC-exosomes (produced from bone marrow mesenchymal stem cells) carry out the same functions as normal BMSCs by significantly reducing neuroinflammation and neuroglial overactivation in animal models, hence improving the overall symptoms of AD. As well there was a significant decrease in Aβ1−42, and tau.
In the case of ESCs, one of the main issues was problems with immunorejection from the patient, making it an ineffective treatment. However in the case of MSCs, some studies show that they may have immunomodulatory effects and can therefore suppress effects on T-cell proliferations. This may be extremely helpful in solving the issue with immunorejection after MSC transplants.
MSCs have proven to be safe options for Alzheimer's disease therapy but their effectiveness has yet to be decided. After 17 clinical trials of MSCs, all of which were during the early phase of the disease, and 5 relevant outcomes, MSCs are considered to be safe and likely can be used for AD therapy. Due to small size of subjects, variations in dosage, MSCs source, and administration scheme (route, timing, and frequency), MSC efficacy has not been proven yet. Overall there needs to be some better trials to determine a solid outcome.
INDUCED PLURIPOTENT STEM CELLS
In 2006, a groundbreaking study was published by Yamanaka about reprogramming cells to become pluripotent cells. Mainly derived from mouse embryonic or adult fibroblasts through introducing four factors; Oct3/4, Sox2, c-Myc, and Klf4. Hence, this process is called “induced pluripotent stem (iPS) and was created through embryonic stem cell conditions. For his work, Yamanaka was awarded the 2012 Nobel Prize in Medicine. Yamanaka's trial stood out because previously inducing somatic cells to reprogram into iPSCs required the use and introduction of genetic material that originated outside of the human body. This would mean the overexpression of certain transcription factors for protein synthesis leading to overall dedifferentiation. As well, introducing these genes may lead to the development of tumors within the new, stem cell created tissue. To counteract this, a protein based method for inducing pluripotency without genetic modifications was suggested. This increased safety compared to previous methods.
The differentiation ability of iPS cells are believed to be equivalent to ESC with the added benefits of minimizing immunogenic and ethical issues.
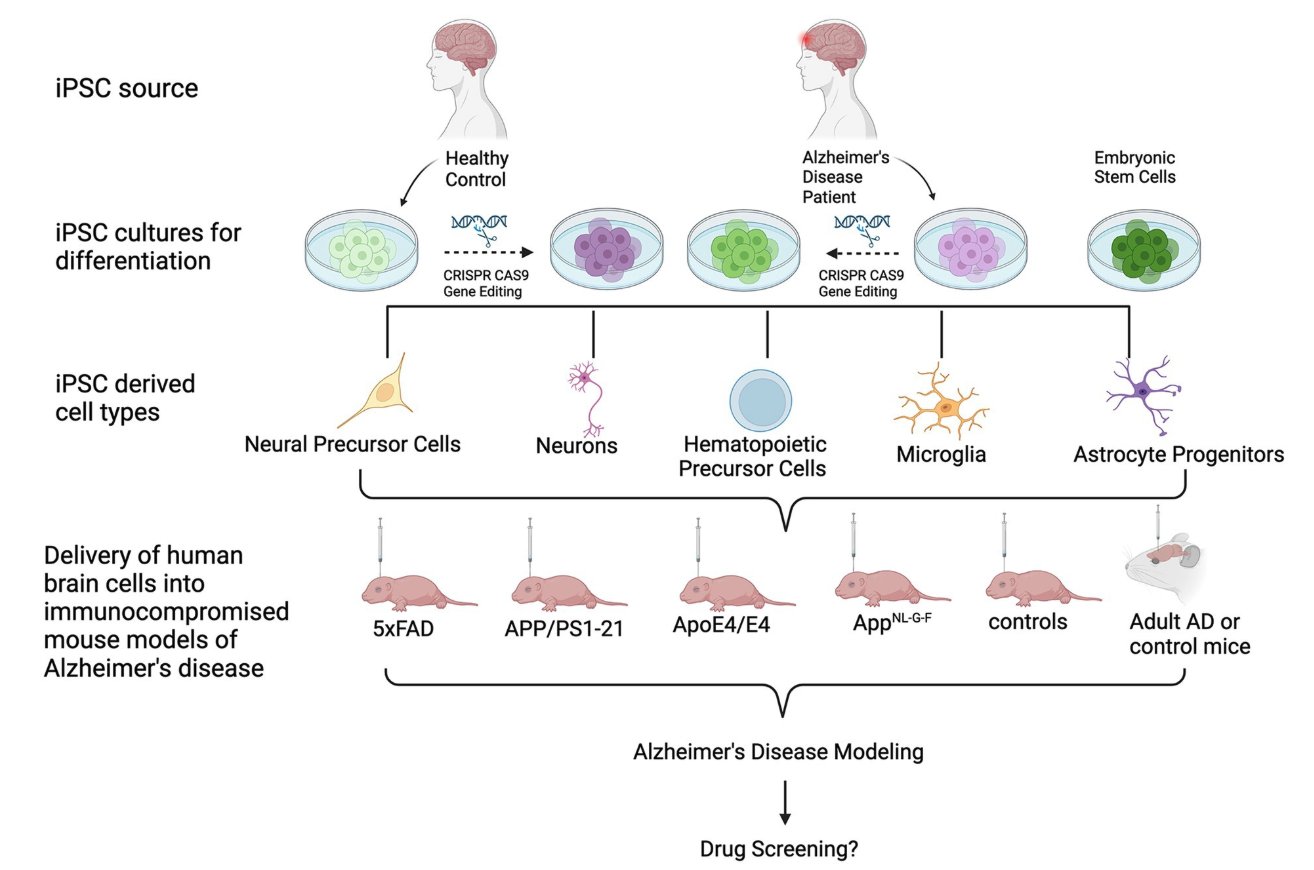
Researchers Moon-Yong Cha discovered that transplanting Protein-iPSCs into transgenic AD mouse models resulted in differentiation of glial cells along with decreased plaque formation and cognitive impairment overall. Conversely, the research group of Edsel M. Abud found that microglia-like cells (iMGLs) that actually differentiated from iPSCs grow in vitro similar to how microglia grow in vivo. They also planted iMGLs into human brain organoids and mice brains and found that the iMGLs resembled microglia. This is better than the abnormal microglia that is associated with neuroinflammation and tau tangled. Normal microglia naturally protect the brain from amyloid-beta plagues. Since intracerebral delivery of iPS, mice have had results with a significant decrease of Aβ levels in interstitial fluids.
CLINICAL TRIALS
Some clinical trials have also been performed with the four given stem cells though they primarily focused their research on the Phase 1 or Phase 2 of AD, mainly to assess effectiveness and stem cells preparations.
Hee Jin Kim conducted two clinical trials with mesenchymal stem cells during phase 1 of AD. He wanted to test appropriate dosage and limiting toxicity of stereotactic intracerebral injection of MSCs that are derived from human umbilical cord blood (hUCB-MSCs). It was injected directly into the hippocampus. The patients overall did not experience any serious effects from the injection during the 24 month follow-up period.
As well, after this, Hee Jin Kim conducted a study to assess safety and dose limiting toxicity of three ventricular injections. He did this through insertion of an Ommaya reservoir which is a soft, plastic made reservoir giving direct access to cerebrospinal fluid. hUCB-MSCs was injected into three stem cell injections administered to the patient over the span of four weeks, equally separated. The patients were monitored for up to 12 weeks, and then another 36 weeks to determine results for an extended study. hUCB-MSC administration through the lateral ventricle was determined to be relatively safe, the only most common symptom was fever. Five patients completed the study without feeling any additional symptoms or effects. These two trials stood out for their significant results.
ETHICS, CHALLENGES AND NEGATIVE OUTCOMES
Overall, there are many challenges with Alzheimer's Disease, which is why there have been so many regulations around testing and using stem cells.
With ESC’s the main issue is ethics and being able to obtain ESCs from the blastocyst. Obviously the process is very controversial and unethical, which is why ESCs have not been used for clinical trials. As well, often ESC causes natural immune rejection from the body, therefore making it more unhelpful.
There is also an overall lack of clinical trials testing for effectiveness and success of stem cells. As well I believe that mouse models need to be improved to better reflect the human brain for there to be any viable proof. This became the main problem with NSCs where the mice models did not accurately reflect the human brain in terms of pathology. Because of this it was hard to pinpoint the benefits of NSC transplants. Tumours and tumour growth was the main prevalent issue with NSC treatment, which is likely why it has not yet been approved for clinical trials and treatment. It is to be noted that MSC’s also have a risk of tumorigenesis but it is significantly less than that of NSCs
Cost of treatment, informed consent and autonomy and long-term effectiveness are important issues to take into consideration as well.
Data
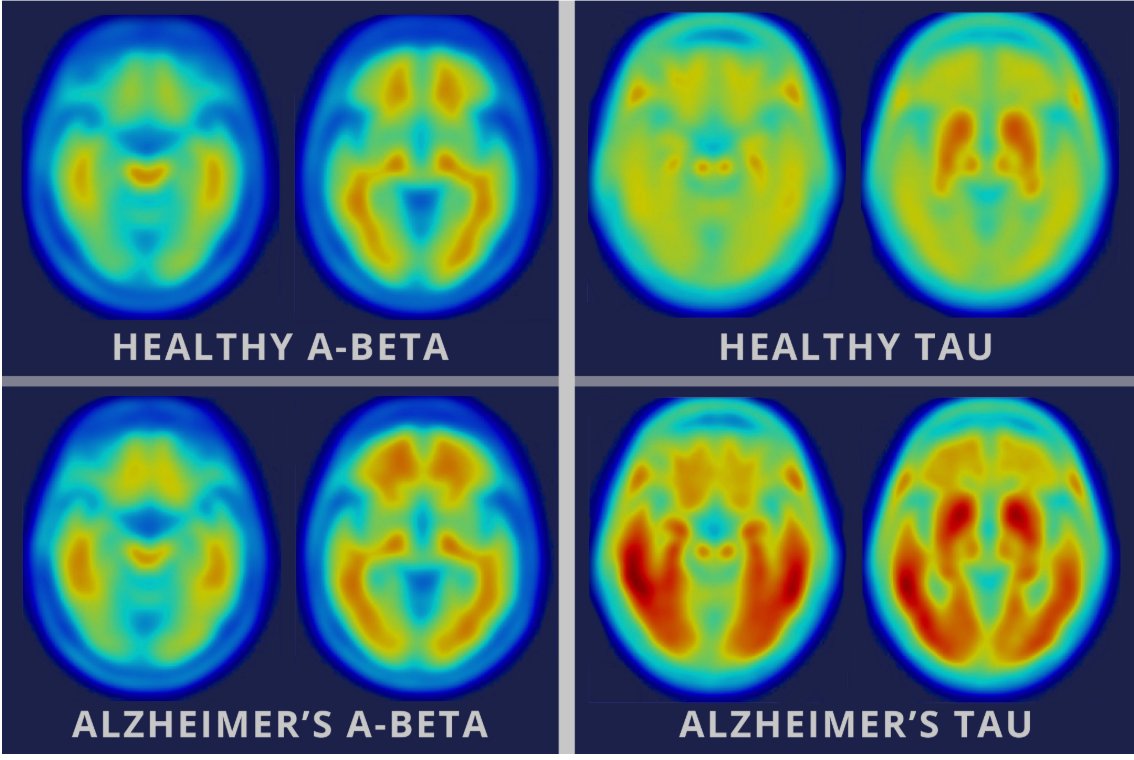 https://medcitynews.com/2016/05/brain-imaging-agent-alzheimer/
https://medcitynews.com/2016/05/brain-imaging-agent-alzheimer/
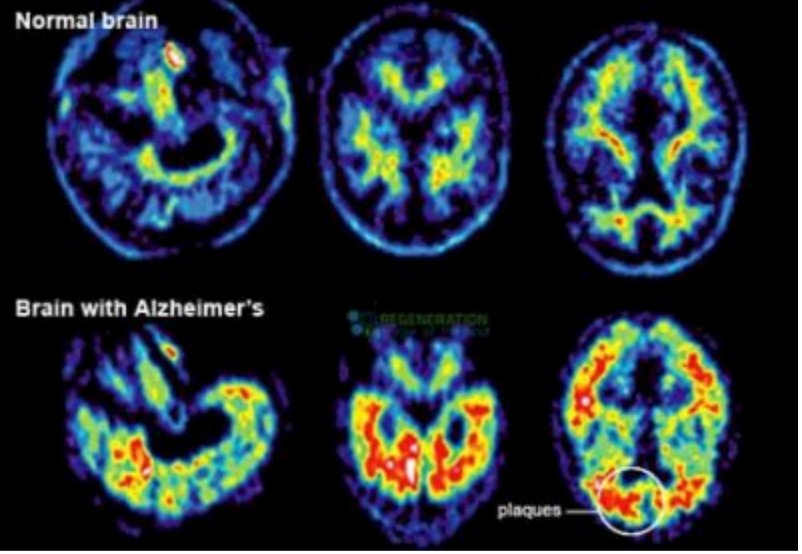 https://stemcellthailand.org/therapies/alzheimers-dementia/
https://stemcellthailand.org/therapies/alzheimers-dementia/
Stages of Alzheimer’s Disease Table
| Stage | Symptoms |
|---|---|
| Stage 1 |
|
| Stage 2 |
|
| Stage 3 |
|
| Stage 4 |
|
| Stage 5 |
|
| Stage 6 |
|
| Stage 7 |
|
This graph is provided from the source https://alzheimer.ca/sites/default/files/documents/Progression-Overview-Alzheimer-Society.pdf
 https://www.sciencedirect.com/science/article/abs/pii/S0306452224003324
https://www.sciencedirect.com/science/article/abs/pii/S0306452224003324
 https://www.sciencedirect.com/science/article/pii/S0014488619302596
https://www.sciencedirect.com/science/article/pii/S0014488619302596
 https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2024.1354164/full
https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2024.1354164/full
Conclusion
Due to the lack of pathological and pathophysiological conclusions around Alzheimer’s disease, ex debate over the role of Aβ plaques and tau, there is hardly enough information to make a concrete treatment. The Vascular Thesis is a prime example of the lack of knowledge and research around Alzheimer's. As well, the disparities between mice models and human brains needs to be filled to properly understand and continue research around stem cell treatment. This way we can continue to improve Alzheimer therapy research and create even better treatments.
However, due to the many significant positive trials, I believe that stem cells are definitely still a viable treatment for Alzheimer’s and have the capabilities of slowing the deterioration of the brain. Unfortunately, at this point I believe stem cells do not have the capacity to cure Alzheimer's, but instead significantly decrease the rate of dementia. This is mainly because of the inherent limiting factors around stem cells such as having enough to actually overpower the deteriorating cells. This, I think will take a substantial amount of time and further research to actually achieve a point where stem cells can be a cure of Alzheimer's.
Though MSC’s are the best current treatment option, there are issues revolving around accessing and finding MSC’s for treatment. This is because a patient would have to rely on a donor to receive cells from their bone marrow, which has ethical concerns and can be inefficient. Technically there are no issues with MSC administration since they naturally are effective intravenously, which is likely also the most efficient method. They are able to naturally follow areas of neuroinflammation within the brain whereas NSCs would have to be surgically implanted, which is a major reason why they are a better option than MSCs. NSCs require stereotactic surgery (invasive brain surgery) to be administered which is why they are highly inefficient.
iPSCs have proven to have the most potential as a treatment method but are yet to be allowed and clinically tested for use. Referencing Yamanaka's discovery, I believe the most effective treatment method would be to turn iPSCs into MSCs, likely using biochemical engineering methods to do this. This way we can eliminate the issue of finding MSC’s to use from human bone marrow and instead cultivating replicas within a petri dish. Though this may be a more costly method, it is much more effective and efficient. It further eliminates any ethical issues surrounding taking MSCs from bone marrow, therefore we are not necessarily reliant on donations.
In conclusion, currently stem cells are not a cure for Alzheimer's Disease but will play a much better impact on delaying brain deterioration and fixing associated symptoms than any drugs do as of right now. I feel that converting iPSCs into MSCs and then using those for treatment is the most effective method and will remove many of the significant limitations around normal human derived MSCs.
Citations
Altodia. (2022, July 5). Understanding The Stages: Preclinical Alzheimer's Disease. Altodia. https://altoida.com/blog/understanding-the-stages-preclinical-alzheimers-disease/#:\~:text=Preclinical%20Alzheimer's%20disease%20begins%20when,the%20onset%20of%20clinical%20symptoms Alzheimer Society. (2026, N/A N/A). The stages of Alzheimer's disease. Alzheimer Society. https://alzheimer.ca/en/about-dementia/what-alzheimers-disease/stages-alzheimers-disease?gad_source=1&gad_campaignid=20672173573&gbraid=0AAAAADwntYFOD9SrLOyJl4Pd8nXMwkNjz&gclid=Cj0KCQiA7-rMBhCFARIsAKnLKtBYC2cjlMTxU5aZF284L2ODePuy_tN09CqlOHhrUjp8uZzkppDarKw Alzheimer's Stages - Early\, Middle\, Late Dementia Symptoms | alz.org. (n.d.). Alzheimer's Association. Retrieved March 3\, 2026\, from https://www.alz.org/alzheimers-dementia/stages Amyloid Beta Peptide - StatPearls - NCBI Bookshelf. (2025, April 27). NCBI. Retrieved March 3, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK459119/ Bhatt, A., Bhardwaj, H., & Shrivastava, P. (2024, September 13). Mesenchymal stem cell therapy for Alzheimer’s disease: A novel therapeutic approach for neurodegenerative diseases. ScienceDirect. https://www.sciencedirect.com/science/article/abs/pii/S0306452224003324 Boese, A. C., Lee, J.-P., & Hamblin, M. H. (2019, November 24). Neural stem cell therapy for neurovascular injury in Alzheimer's disease. ScienceDirect. https://www.sciencedirect.com/science/article/pii/S0014488619302596 Differential expression of cholesterol hydroxylases in Alzheimer's disease - PubMed. (2004, August 13). PubMed. Retrieved March 3, 2026, from https://pubmed.ncbi.nlm.nih.gov/15148325/ Frazer, G. (2025, March 9). ‘Silent Phase’ of Alzheimer’s Begins Decades Before Symptoms. Pacific Hearing Inc. ‘Silent Phase’ of Alzheimer’s Begins Decades Before Symptoms Human stem cell transplantation models of Alzheimer's disease. (n.d.). Frontiers. Retrieved March 3, 2026, from https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2024.1354164/full Induced Pluripotent Stem Cells for Treatment of Alzheimer's and Parkinson's Diseases. (2022, January 19). PMC. Retrieved March 3, 2026, from https://pmc.ncbi.nlm.nih.gov/articles/PMC8869146/#sec4-biomedicines-10-00208 Induced Pluripotent Stem Cells for Treatment of Alzheimer's and Parkinson's Diseases. (2022, January 19). PMC. Retrieved March 3, 2026, from https://pmc.ncbi.nlm.nih.gov/articles/PMC8869146/#sec4-biomedicines-10-00208 Kaminska, A., Radoszkiewicz, K., Rybkowska, P., Wedzinska, A., & Sarnowska, A. (2022, April 26). Interaction of Neural Stem Cells (NSCs) and Mesenchymal Stem Cells (MSCs) as a Promising Approach in Brain Study and Nerve Regeneration. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC9105617/#:\~:text=However%2C%20their%20application%20is%20limited,of%20the%20neural%20cell%20niche. Levy, S., Korbulic, H., & Cohen, D. (2016, May 13). New brain imaging agent is marker for progression of Alzheimer's. MedCity News. Retrieved March 3, 2026, from https://medcitynews.com/2016/05/brain-imaging-agent-alzheimer/ Miao, J., Ma, H., & Yang, Y. (2023, June 15). Microglia in Alzheimer’s disease: pathogenesis, mechanisms, and therapeutic potentials. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC10309009/#:\~:text=Alzheimer's%20disease%20(AD)%20is%20a%20progressive%20neurodegenerative%20disorder%20characterized%20by,crucial%20for%20developing%20effective%20treatments. Neural Stem Cells in the Treatment of Alzheimer's Disease: Current Status, Challenges, and Future Prospects. (2022, November 2). PMC. Retrieved March 3, 2026, from https://pmc.ncbi.nlm.nih.gov/articles/PMC10473082/ Neural Stem Cells in the Treatment of Alzheimer's Disease: Current Status, Challenges, and Future Prospects. (2022, November 2). PMC. Retrieved March 3, 2026, from https://pmc.ncbi.nlm.nih.gov/articles/PMC10473082/ Neural Stem Cell Therapy for Alzheimer's, Vascular & Lewy body. (n.d.). The Regeneration Center. Retrieved March 3, 2026, from https://stemcellthailand.org/therapies/alzheimers-dementia/ Neuroinflammation: What Many Brain Diseases Have in Common. (2025, January 13). American Brain Foundation. Retrieved March 3, 2026, from https://www.americanbrainfoundation.org/what-is-neuroinflammation/ Novartis. (2018, August 21). Neuroscientists target Alzheimer’s “silent stage”. Novartis. https://www.novartis.com/stories/neuroscientists-target-alzheimers-silent-stage#:\~:text=Research%20exploring%20the%20first%20visible,need%20to%20remain%20cognitively%20healthy Ou, C.-M., Xue, W.-W., Liu, D., Ma, L., Xie, H.-T., & Ning, K. (2024, November 20). Stem cell therapy in Alzheimer’s disease: current status and perspectives. frontiers. https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2024.1440334/full?utm_source=twitter&utm_medium=social&utm_content=&utm_campaign=imp_impartaut-_05-24_fnins_en_n--ww OVERVIEW. (n.d.). Alzheimer Society. Retrieved March 3, 2026, from https://alzheimer.ca/sites/default/files/documents/Progression-Overview-Alzheimer-Society.pdf Pazili, T. H. (2024, July 15). A Severe Alzheimer's Disease Patient Improved by Intravenous Mesenchymal Stem Cell Transplant. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC11262880/#:\~:text=4.,in%20other%20various%20neurological%20diseases. Poliwoda, S. (2022, August 25). Stem cells: a comprehensive review of origins and emerging clinical roles in medical practice. PMC. Retrieved March 3, 2026, from https://pmc.ncbi.nlm.nih.gov/articles/PMC9404248/ The Role of Tau in Alzheimer's Disease and Related Disorders. (n.d.). PMC. Retrieved March 3, 2026, from https://pmc.ncbi.nlm.nih.gov/articles/PMC4072215/ Stem cell therapy offers new hope for the treatment of Alzheimer's disease. (n.d.). Frontiers. Retrieved March 3, 2026, from https://www.frontiersin.org/journals/cell-and-developmental-biology/articles/10.3389/fcell.2025.1650885/full Therapeutic Efficacy of Mesenchymal Stem Cells (MSCs) on Alzheimer's Disease: Review of Clinical Results. (2026, January 15). PubMed. Retrieved March 3, 2026, from https://pubmed.ncbi.nlm.nih.gov/41533329/ Xu, Y., & Gao, W. (2023, December 22). New insight on microglia activation in neurodegenerative diseases and therapeutics. National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC10770846/#:\~:text=4.,function%2C%20and%20induction%20of%20neuroinflammation
https://www.alz.org/alzheimers-dementia/stages
https://alzheimer.ca/sites/default/files/documents/Progression-Overview-Alzheimer-Society.pdf
https://pmc.ncbi.nlm.nih.gov/articles/PMC4072215/
https://www.americanbrainfoundation.org/what-is-neuroinflammation/
https://pmc.ncbi.nlm.nih.gov/articles/PMC10473082/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8869146/#sec4-biomedicines-10-00208
https://pmc.ncbi.nlm.nih.gov/articles/PMC8869146/#sec4-biomedicines-10-00208
https://medcitynews.com/2016/05/brain-imaging-agent-alzheimer/
https://stemcellthailand.org/therapies/alzheimers-dementia/
https://www.sciencedirect.com/science/article/abs/pii/S0306452224003324
https://www.sciencedirect.com/science/article/pii/S0014488619302596
https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2024.1354164/full
Acknowledgement
I would like to acknowledge my Biology teacher Mrs. Calvert from Master's Academy and College for supporting me through the creation of my project and helped me kickstart a CYSF Science Fair Club at my school.