
Closing the Perception Gap: Smartphone UV Detection as a Behavioral Intervention for Sunscreen Misapplication
Heer Joshi
James Fowler High School
Grade 11
Presentation
Problem
Every summer, millions of people believe that they are protected from harmful UV radiation because they applied sunscreen. But they are wrong. Research shows consumers apply only 20-50% of the recommended amount (Petersen & Wulf, 2014), yet they remain completely unaware of this deficit. This creates the "SPF Illusion" , a false confidence in insufficient protection that persists despite decades of education campaigns. The problem is not the lack of knowledge. Studies prove that even medical students who understand sun safety apply inadequately, with only a 0.216 correlation between knowledge and proper practice (Genaro et al., 2018). In Sweden, 68% of people correctly attribute skin cancer to sun exposure, yet 85% refuse to change their sunbathing behavior (Bränström et al., 2005). Why? Because UV radiation is invisible, people cannot see where they have missed, cannot verify adequate thickness and receive no immediate feedback to correct their mistakes.
This is not negligence. It is a human sensory limitation combined with psychological biases:
- Dunning-Kruger Effect: Familiarity creates false expertise ( I have done this 1,000 times, I am good at it)
- Optimism Bias: It won't happen to me (17% of men believe their skin cancer risk is below average despite no justification)
- Sensory limitation and SPF Rating Illusion: High numbers (SPF 50, 100) create false security regardless of application quality.
- Confirmation Bias: Feeling sunscreen on skin is interpreted as evidence of complete coverage
- Temporal Disconnect: Sunburn appears hours later, cancer decades later - no immediate learning feedback.
The result? Laboratory SPF testing assumes 2 mg/cm², but real consumers apply 0.39-1.0 mg/cm². An SPF 50 sunscreen applied at typical thickness provides protection closer to SPF 10-15. This showcases that users are not aware that this is occurring.
Evidence:
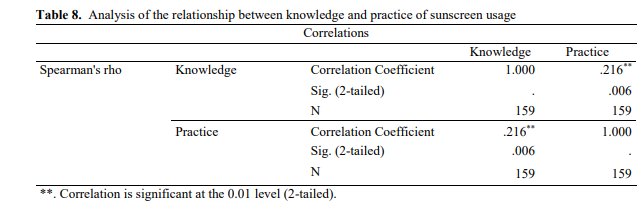
This data was written by the medical students to study a behavior of sunscreen usage among them. This data showcases that people have knowledge of the application of sunscreen but the application of it is the main issue. We can see it by the difference of coefficient in it.
Figure 1: Analysis of the relationship between knowledge and practice of sunscreen usage
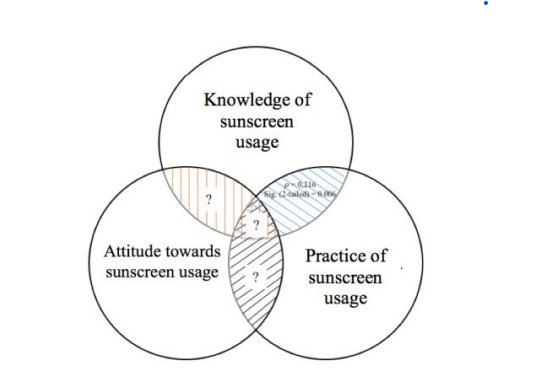
While the medical students study successfully established that knowledge of sunscreen usage does not correlate strongly with correct practice, it left two fundamental questions unresolved: the root cause of this disconnect and a viable solution to bridge it. This project was designed specifically to investigate and answer both.
Figure 2: Venn Diagram of Sunscreen Usage amoung people
Method
MY HYPOTHESIS: The Perception Gap Exists and Is Measurable
If a smartphone-based UV imaging system is used to visualize sunscreen application in real time, then users will achieve measurably more complete UV protection coverage than those applying without visual feedback, because human eyes are biologically incapable of detecting ultraviolet wavelengths, leaving people unable to identify missed areas through any natural sensory means which leads to chronic underprotection and significantly increased risk of melanoma over time.
I built a functional UV imaging prototype using modified consumer hardware to prove the concept, then propose smartphone integration as the scalable solution for population-wide impact.
WHAT I DID?
- People Tested: 15
- Demographics: Mixed gender
- Recruitment: Family and friends
- Limitation: Only hands were tested to get a similar result and to find commonly missed spots
Procedure
- Participants received instructions to apply sunscreen to their hands as they normally would for sun protection.
- No specific guidance on amount or technique was provided to capture their application behavior.
- Self-Assessment (Before UV Verification) Participants completed a brief questionnaire, it asks for how confident are they in their sunscreen application quality? (1-10 scale, where 1=not confident, 10=very confident).
- Then, participants hands were examined under our UV camera.
- UV illumination revealed:
- Dark areas = sunscreen present (UV absorption)
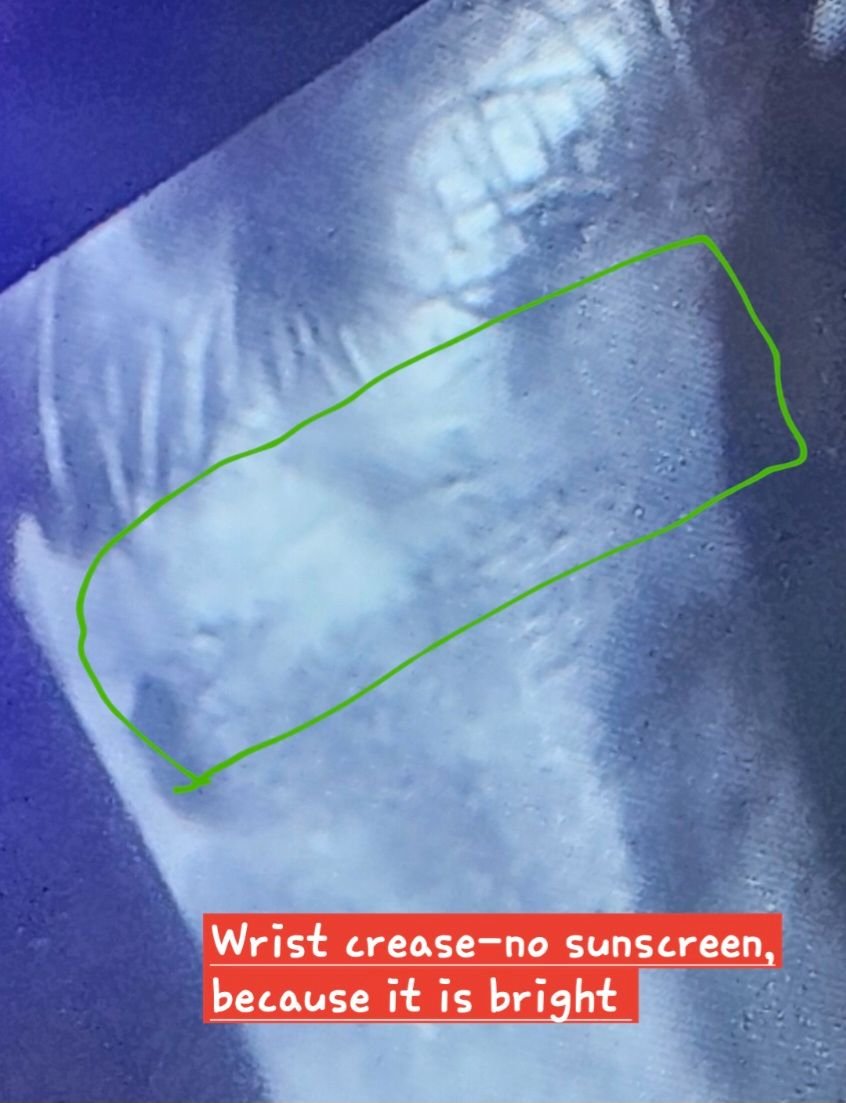
- Bright areas = bare skin (missed areas)
- Commonly missed areas were documented:
- Between fingers
- Knuckles
- Fingernails/cuticles
- Wrist creases
- Back of hand edges
- : Post-UV Assessment-After viewing their UV-illuminated hands, participants were asked the same question again:
- Confidence level (After): How confident are you now in your original application? (1-10 scale)
- Immediate reactions: responses were recorded
- Then a technology interest question were asked: Would they use a smartphone UV detection feature if available? (Yes/No)
- At the end I did perception gap calculation.
How was UV camera made?
Imagine trying to verify something you literally cannot see. That is the problem with sunscreen, it protects against ultraviolet radiation, which is completely invisible to human eyes. UV light exists just beyond violet on the electromagnetic spectrum, with wavelengths between 280-400 nanometers. Our eyes only detect wavelengths between 400-700 nanometers, making UV as invisible to us as radio waves. This means when you apply sunscreen, you are trying to verify protection against something you cannot perceive. It is like trying to check if you closed all the windows in your house while blindfolded, you might feel confident you got them all, but without seeing, you can't actually know.
Professional UV cameras that reveal sunscreen coverage exist, but they cost $200-300, putting them out of reach for most people. I realized that if UV detection technology remained expensive and inaccessible, my research findings no matter how significant, would remain an interesting curiosity rather than a practical solution. So I decided to build my own UV camera from scratch using modified consumer hardware, proving that this technology could be made affordable enough for everyone. What follows is the story of how I transformed a $15 webcam into a specialized scientific instrument capable of revealing hidden ultraviolet patterns.
While researching construction methods for my UV camera, I came across a DIY infrared night vision camera project by Project 326, which demonstrated how a standard USB camera module could be modified by removing its built-in filter and replacing it with a different optical filter to capture invisible wavelengths of light. This video became a key reference point for my build, as the process of modifying a UV camera follows the same fundamental principle the only difference was the type of filter used. Seeing this infrared build confirmed that my approach was not only scientifically sound but practically achievable with accessible, low-cost consumer hardware.
The secret- Silicon sees what we cannot
I found something surprising that your smartphone camera can already detect UV light. The silicon sensors inside digital cameras are naturally sensitive to ultraviolet wavelengths, they just need permission to see them. Silicon is a semiconductor material that responds to photons (light particles) across a broad spectrum. When UV photons hit silicon, they have enough energy to knock electrons loose, creating an electrical signal. This is exactly how the camera detects visible light too, just at different wavelengths.
So why don't normal cameras show UV? Because manufacturers don't want them to. UV contamination ruins regular photos by creating haziness, weird color shifts and blurriness. To prevent this, they install special filters over the sensor that block UV and infrared while letting visible light through. It is same as the concept like wearing sunglasses that filter out glare, you see a clearer, more natural image of the world. But for my purposes, I needed to remove them and install the opposite filter that blocks visible light but lets UV through. This would transform the camera from seeing what humans see into seeing what humans cannot.
The Building
I ordered a simple USB camera module online, the kind used for basic webcams and Raspberry Pi projects. When it arrived, I was holding in my hands a piece of technology that could already detect UV light; it just did not know it yet. The modification process would be delicate. I was essentially performing surgery on a tiny electronic device and one wrong move could destroy the sensitive image sensor inside.
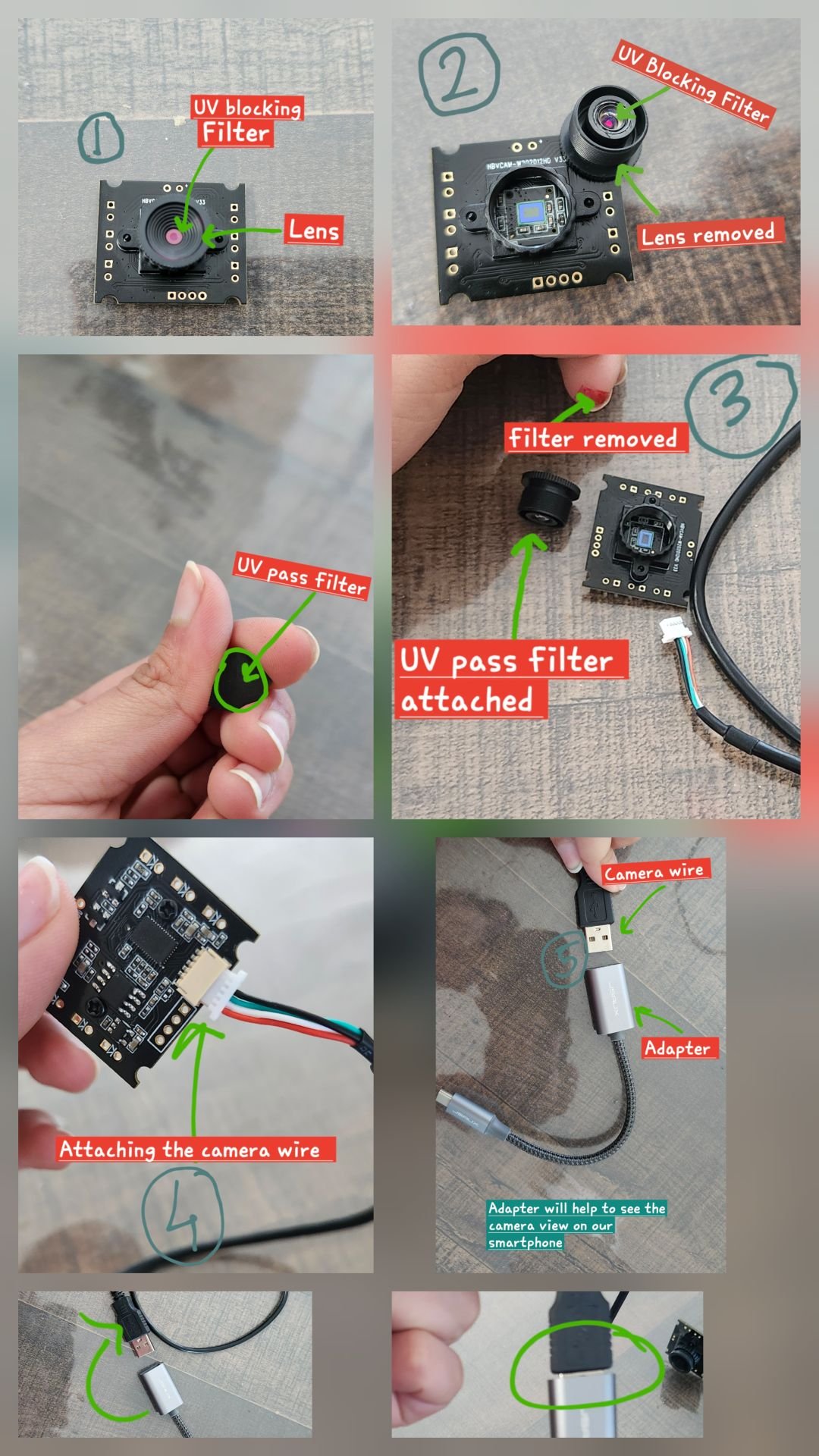
Step 1: The Disassembly
I carefully removed the tiny screws holding the camera housing together. Inside, I found a small circuit board with the image sensor, a square chip about the size of my pinky fingernail. Above the sensor sat the lens assembly and directly on top of the sensor itself was a thin optical filter that looked like a tiny square of tinted glass. This was the UV-blocking filter that had to go. The hardest part was removing this filter without damaging the sensor beneath it. The sensor surface is incredibly delicate, any scratch, fingerprint or speck of dust would create permanent defects in every image. Using tweezers and working under a magnifying glass, I carefully scored the adhesive holding the filter in place, gradually loosening it. After several tense minutes of gentle prying, the filter came free. I set it aside and stared at the exposed sensor surface, knowing that what happened next would determine whether this experiment succeeded or I just destroyed a camera.
Step 2: The precaution With the sensor exposed, I had to work fast to minimize dust exposure.
Step 3: The UV Filter Installation Now came the moment of truth, installing the UV-pass filter. This specialized optical filter does the opposite of what I just removed, it blocks visible light (everything you can see with your eyes) and infrared, but allows UV wavelengths between 320-400 nanometers to pass through. I had ordered this filter specifically for UV imaging applications.
Using tweezers, I lowered the filter into position, ensuring it was level and centered. There was no going back because any adjustment would risk contaminating the sensor or misaligning the filter. Then, I gently pressed the filter's edges to seat it properly.
Step 4: Final step- testing UV camera I reassembled the camera housing and connected it to my smartphone via USB adapter. I had prepared a test target, a piece of white paper with half covered by a thick layer of sunscreen. I positioned that paper in sunlight to illuminate the paper, then opened the camera software. What I saw on screen was the half of the paper without sunscreen glowed bright white, the paper was reflecting UV light directly back to the camera. But the half with sunscreen appeared dark, almost black, the sunscreen was absorbing the UV, preventing it from reaching the camera. The contrast was stunning, far clearer than I hoped. I had done it. My modified $15 camera could reveal the invisible world of ultraviolet radiation.
Figure 3:
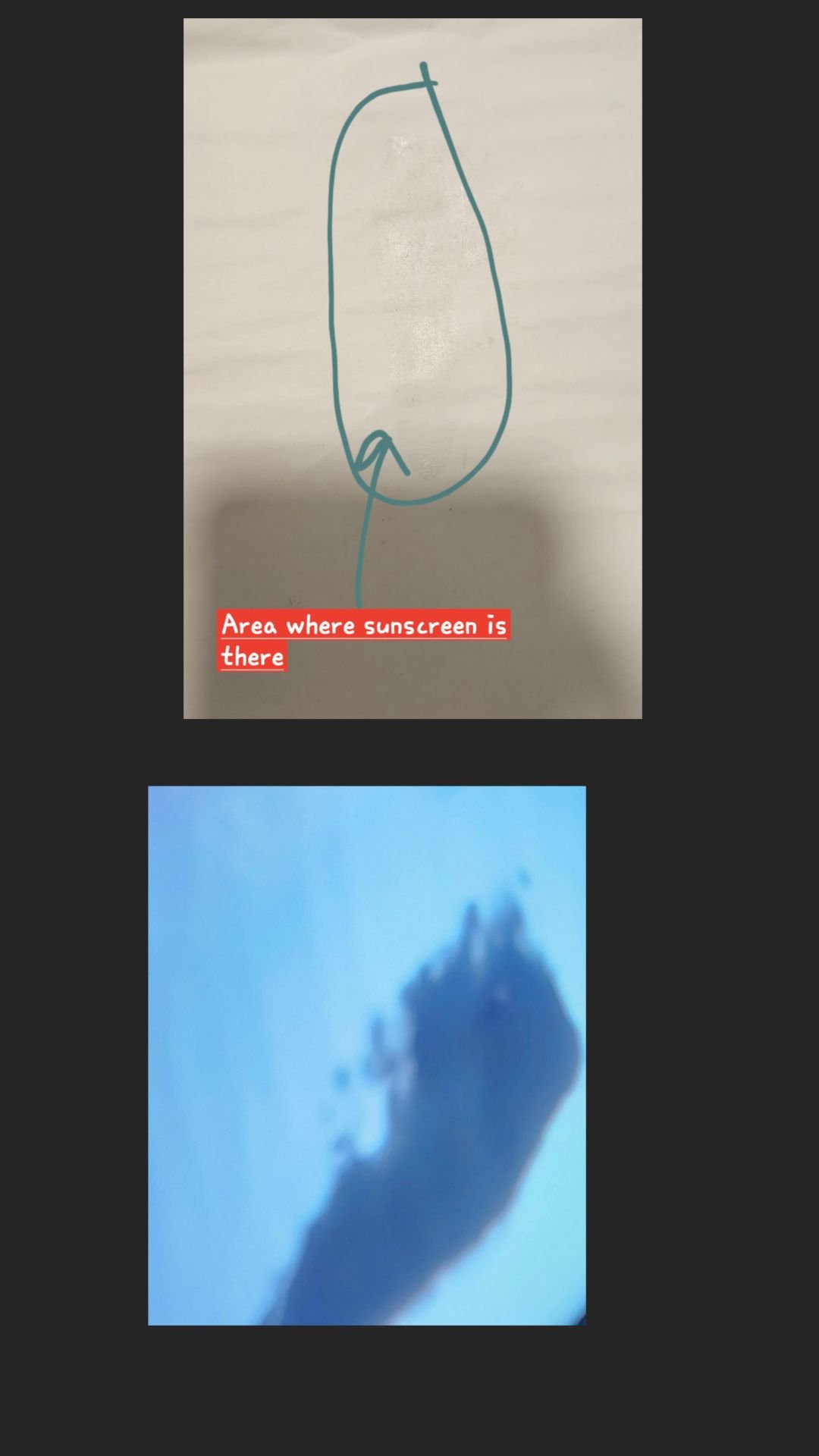
Figure 4:

Figure 5: Building of UV camera Images
Testing on Real Skin: The First Revelation
I applied sunscreen to my own hand, rubbing it in the way I normally would. My hand looked covered, I felt confident I have done a thorough job. Then I held my hand under the sunlight and viewed it through the modified UV camera. Bright white patches glowed between my fingers, across my knuckles, around my fingernails, everywhere I had unconsciously missed or applied too thinly. The areas where I did actually achieved adequate coverage appeared dark, creating a patchwork pattern of protection and exposure I have been completely unaware of. I was looking at my own perception gap in real-time and it was shocking. If I, someone who had spent weeks researching sun safety and knew exactly what I was looking for had missed this much coverage, what did that mean for everyone else? This moment crystallized the entire purpose of my project. I was not just conducting an experiment, I was proving that a technology which should be in everyone's hands could be built affordably from basic components. If I could transform a $15 camera into a UV imaging system in my bedroom, smartphone manufacturers with billion-dollar Research and development budgets could certainly integrate UV detection into their devices. I had my proof of concept and it worked beautifully.
Figure 6:
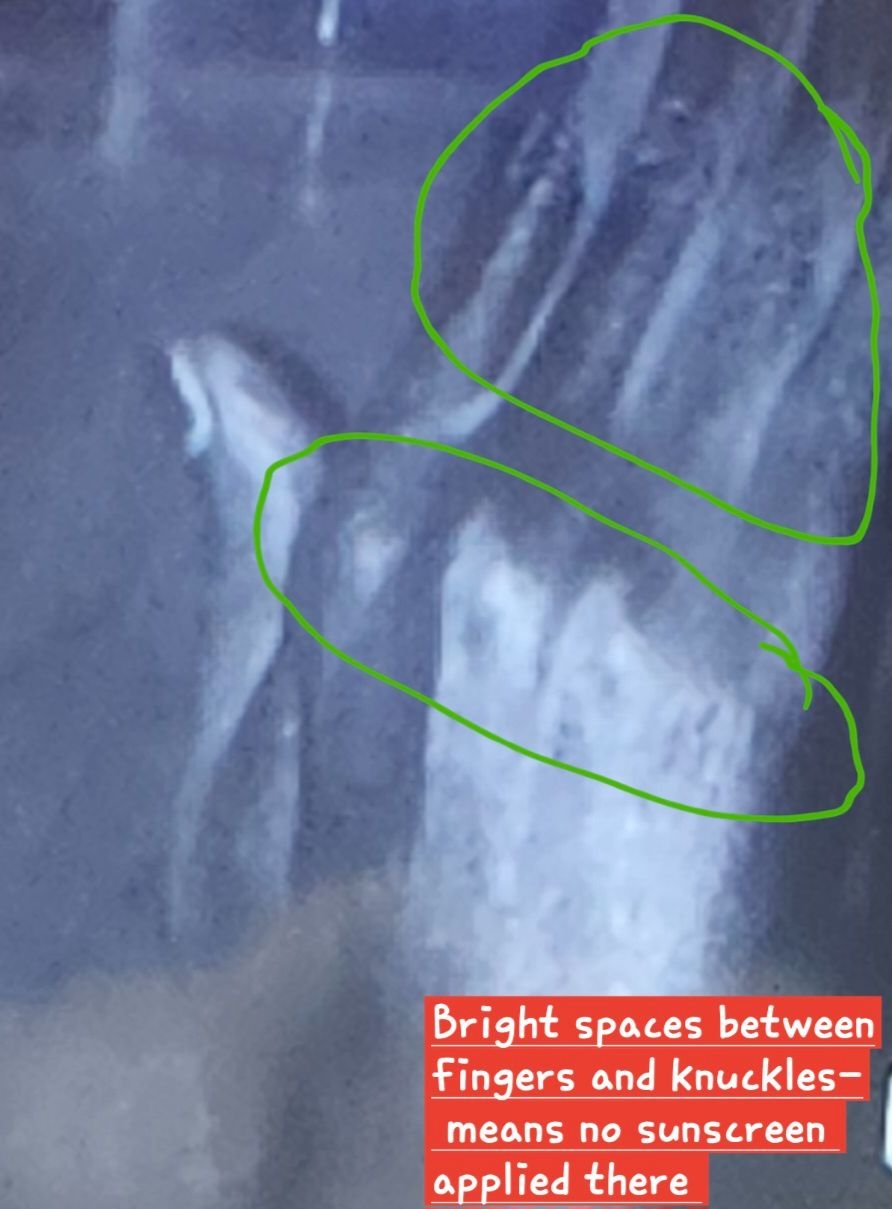
Figure 7:
Analysis
Results:
- Average perceived coverage (before UV): 74%
- Average actual coverage (after UV): 40%
- Perception gap: 34%
- Participants who overestimated: ALL
- Commonly missed areas: Between fingers, Knuckles, Fingernails/cuticles, Wrist creases, Back of hand edges
- The reaction: Participants genuinely believed they did applied thoroughly until seeing their hand glow under UV camera with obvious gaps.
- Solution interest was high: 100% said they would use a smartphone UV detection feature if available.
Figure 8:
Data:
Table of Confidence Before applying sunscreen VS Confidence After seeing coverage in UV camera
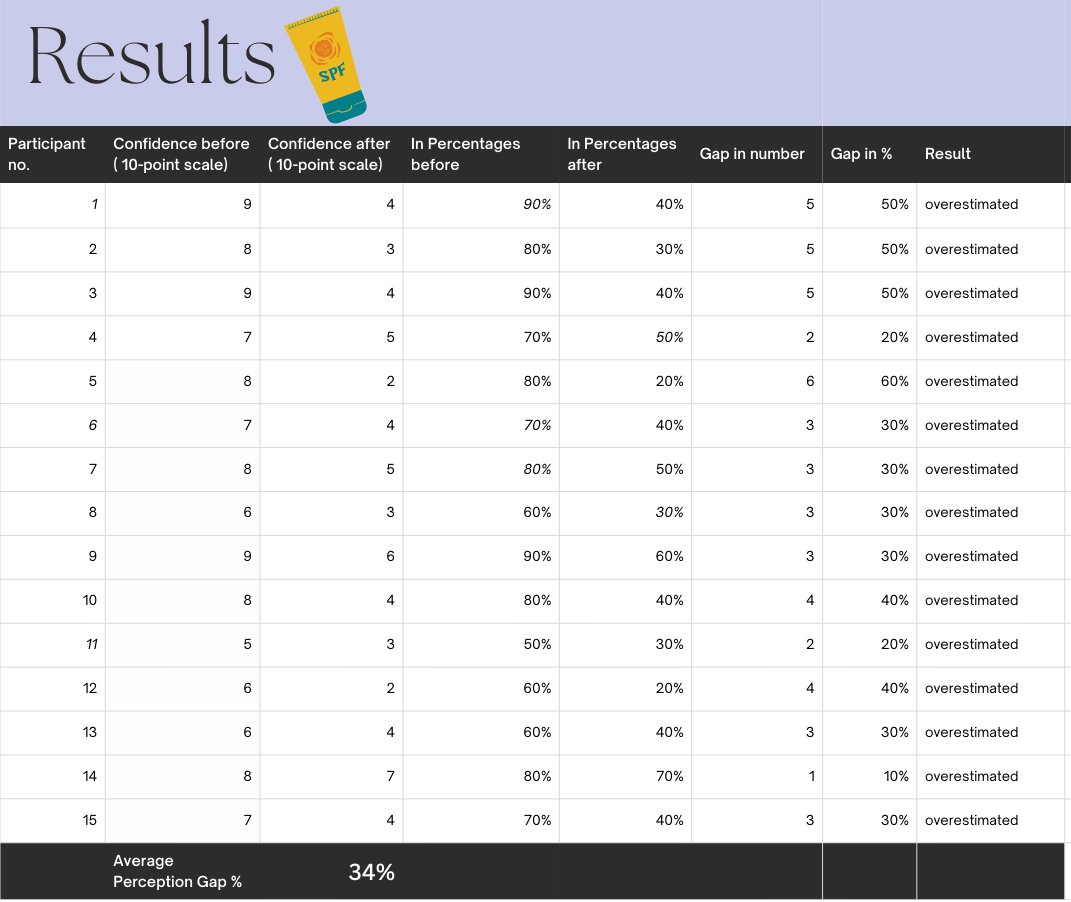
Figure 9:
Graph of Perception gap between Confidence Before applying sunscreen VS Confidence After seeing coverage in UV camera
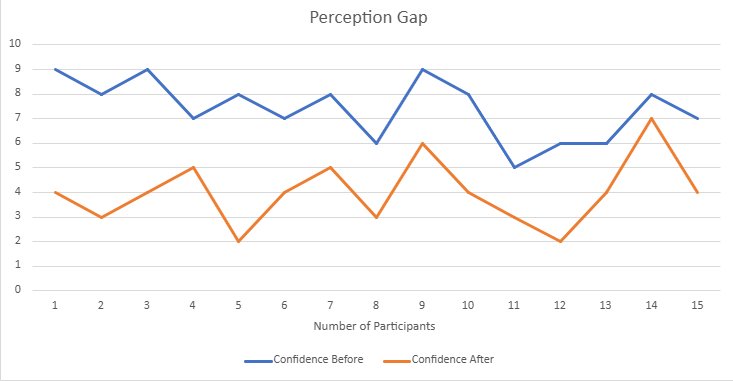
Using my custom-built UV camera, I tested fifteen people aged 16-40, asking each to apply sunscreen to their hands "the way you normally would." Before showing them the UV images, I asked them to estimate what in 10-point scale of their hand they thought was covered. The results were stunning, every single person without exception overestimated how well they had applied sunscreen. Not one person accurately assessed their coverage. Not one person underestimated. Everyone was confidently wrong. On average, participants believed they achieved 74% coverage. Suggesting they thought they have done pretty well with maybe a few small spots missed. The UV camera told a very different story. Their actual coverage averaged just 40%, barely more than half of what they believed. This creates what I call the "perception gap", a 34% difference between what people think they achieved and what they actually achieved. That is not a small error. That is a catastrophic failure of self-assessment that leaves people with approximately half the UV protection they believe they have.
Let me put that in concrete terms, if you apply SPF 50 sunscreen thinking you have covered most of your skin (74%), but you have actually only covered 40%, you are getting protection closer to SPF 25. You are absorbing 46% more UV radiation than you think. Every beach day. Every outdoor activity. Every time you believe you are protected. This accumulated exposure over years and decades dramatically increases melanoma risk, which explains why people who "always wear sunscreen" still develop skin cancer at alarming rates.
Figure 10:

The Universal Pattern: 100% Overestimation
The most striking aspect of these results is their universality. Not a single participant accurately assessed their coverage. Not one person underestimated. Every participant, regardless of their initial confidence level, their sun exposure history or their apparent carefulness during application, overestimated their coverage. This 100% overestimation rate proves beyond doubt that the problem is not confined to careless individuals or poorly educated populations, it is a universal human limitation rooted in our inability to perceive ultraviolet radiation. The consistency of this finding demonstrates that we are observing a fundamental biological constraint rather than correctable behavior. Human eyes detect visible light between 400 and 700 nanometers wavelength, while UV radiation exists between 280 and 400 nanometers, completely outside our sensory capabilities. So, asking someone to verify their sunscreen coverage without UV imaging is basically biologically impossible, regardless of intelligence or education.
Where Everyone Fails: The Missed Areas Map
The UV imaging revealed consistent patterns in exactly where people miss coverage, proving these are not random mistakes but systematic application errors. The data shows clear anatomical patterns in application failure:
- Between the fingers emerged as a critically missed area. When you rub sunscreen into your hands, your fingers are usually pressed together, creating barriers that prevent lotion from reaching those narrow spaces. You feel sunscreen on the sides of your fingers and assume the spaces between must be covered too. But in actual they are not. The UV camera revealed these interdigital spaces glowing bright white in nearly every participant, indicating complete absence of protection in areas that receive significant sun exposure during normal hand use.
- Knuckles showed inadequate coverage in the vast majority of participants. Their curved, bumpy surface causes sunscreen to pool in the valleys while leaving the peaks exposed. Most people rub until they no longer feel wetness and assume they are done. UV imaging reveals the knuckles are still bright white meaning unprotected. This is especially dangerous because knuckles face upward, perpendicular to the sun, receiving maximum UV exposure. The combination of high UV exposure and consistently poor coverage explains why knuckles are such common locations for both sunburn and in older adults, pre-cancerous lesions.
- Around fingernails and cuticles showed frequent gaps. The area immediately surrounding fingernails represents a transition zone that many participants avoided, creating halos of unprotected skin around each nail. The danger of this systematic miss is significant because the nail matrix and surrounding skin are particularly vulnerable to UV damage.
- Wrist creases showed inadequate coverage because sunscreen does not penetrate folds easily. When skin is folded (which occurs naturally at the wrist when the hand is relaxed), the crease itself creates a protected valley where sunscreen cannot easily reach without deliberate spreading of the fold. When the wrist subsequently moves and the skin unfolds during normal activity, these creases flatten out, exposing previously folded (and unprotected) skin to direct sun.
- Back of hand edges showed gaps because people focus on the broad central area of the hand and stop short of the sides, creating a zone of partial or absent coverage around the perimeter.
These consistent patterns prove we are not looking at individual carelessness. These are predictable, systematic failures driven by the mechanics of how people apply sunscreen combined with the fundamental problem that we cannot see if we are actually achieving UV protection. Traditional sun safety advice says "apply thoroughly to all exposed skin," but that generic instruction is of no use when people have no way to verify thoroughness.
The Psychology: Why Everyone Gets It Wrong
The 100% overestimation rate reflects how our brains work when trying to assess something we cannot perceive. First, there is simple sensory limitation. We judge task completion using sensory feedback: we look to see if we have painted all of a wall, we feel to check if our hands are still dirty. But when applying sunscreen, the relevant outcome UV protection happens in wavelengths we literally cannot see. We can see the visible appearance of lotion (white, translucent) and feel its texture (slick, smooth), but neither tells us about UV protection. There is a disconnect between the sensory information available to us and the outcome we are trying to achieve.
This sensory gap gets filled in by confirmation bias, our tendency to interpret information in ways that confirm what we expect. Participants applied sunscreen expecting to be protected, felt sunscreen on their skin and interpreted that sensation as confirmation: "I feel sunscreen, therefore I am covered." But feeling sunscreen presence doesn't confirm adequate thickness or complete coverage. You can feel sunscreen while having massive gaps between your fingers. Confirmation bias prevented people from questioning whether their tactile sensation actually corresponded to adequate protection.
Then there is optimism bias, people believe they are less likely than average to experience negative outcomes. Swedish research found 17% of men believed their skin cancer risk was below average, which is mathematically impossible. This extends to task performance, participants unconsciously assumed "I am probably doing this better than most people" without objective basis. The 74% average perceived coverage essentially says "I did pretty well." Reality disagreed, 40% actual coverage represents failure by any objective standard.
Most insidious is the Dunning-Kruger Effect, familiarity creates an illusion of expertise without actual skill improvement. Years of experience applying sunscreen created familiarity in these participants, familiarity created confidence, but confidence didn't reflect competence. This explains why medical students in Indonesia who understand sun damage better than anyone showed almost no correlation between knowledge and proper application. More education creates more confidence without improving execution because knowledge about why sunscreen matters doesn't provide the feedback needed to detect and correct gaps.
Finally, there is temporal disconnect. Most skills improve through feedback loops, do something, see the result, adjust based on result, improve over time. But sunburn appears 4-8 hours after exposure, too delayed to clearly connect specific application errors to specific burns. Skin cancer appears 20-40 years later, zero learning opportunity. People can apply inadequately thousands of times, experience negative consequences, but never form the causal connection between technique and harm because the feedback is too delayed to be useful.
The Moment of Revelation: Participant Reactions
When participants saw their hands under UV illumination for the first time, their reactions were immediate and visceral. Having just applied sunscreen with what they believed was adequate care, achieving what they estimated as 74% coverage, they expected to see mostly dark (protected) areas with perhaps a few small bright spots indicating minor gaps. What they actually saw shocked them. Their hands lit up with glowing white patches, between every finger, across knuckles, around fingernails, in wrist creases. Areas they had felt confident were well-covered appeared bright white under UV, indicating complete absence of protection. The contrast between their expectation (74% coverage, "I did pretty well") and the visual reality (40% coverage, massive obvious gaps) created immediate cognitive dissonance that was visible in their facial expressions and verbal reactions.
Participants genuinely believed they had applied thoroughly until seeing their hand glow under the UV camera with obvious gaps. The phrase "I can't believe I missed that much" was nearly universal. Several participants immediately asked to try again, wanting to prove they could do better now that they understood where they were failing. Others expressed concern about past sun exposure: "This explains why I always burn on my knuckles even when I use sunscreen" or "I would have gone to the beach like this thinking I was protected."
The psychological impact of this revelation cannot be overstated. Abstract statistics about cancer risk or educational messages about proper application technique had failed to change these participants behavior in the past. But seeing their own skin glowing with UV-exposed gaps, evidence they could observe directly rather than imagine hypothetically, created immediate awareness that their current practice was inadequate. This is the power of making the invisible visible, it transforms understanding from intellectual knowledge ("I should apply sunscreen thoroughly") to visceral recognition ("I can see with my own eyes that where I am failing to protect myself").
Universal Demand: 100% Adoption Interest
When asked whether they would use a smartphone UV detection feature if it were available, every single participant responded affirmatively. This represents 100% adoption interest, a remarkably high rate that reflects the powerful impact of experiencing UV imaging firsthand. Before seeing the UV images, participants had no awareness that a problem existed; they believed their sunscreen application was adequate. After seeing the visual evidence of their coverage gaps, they immediately recognized the need for verification technology.
This universal interest validates a key hypothesis of this project, the primary barrier to adoption of UV detection technology is not resistance to using such technology but rather unawareness that the problem exists. People who have never seen UV imaging of their sunscreen application have no idea they are applying inadequately, therefore see no need for verification tools. However, people who experience UV imaging even once instantly recognize the need because they have personally witnessed their invisible coverage gaps. The 100% adoption interest demonstrates that once people understand the perception gap exists, once they have seen their own hand glowing with missed areas, they immediately want tools to verify coverage.
This finding has profound implications for implementation strategy. It suggests that public demonstrations of UV imaging (at beaches, community health fairs, schools, workplaces) that allow people to experience the revelation firsthand would rapidly create public awareness and demand for UV detection technology. The viral educational video cited, with over 15 million views, demonstrates that there is already substantial public interest in this technology, those millions of viewers now understand the perception gap exists and this study's 100% adoption interest suggests many would actively seek verification methods if available.
Why this solution will work?
UV visualization succeeds where education fails because it addresses the root cause, sensory limitation. Implementation is straightforward users apply sunscreen and view their skin under UV camera. Areas with adequate coverage appear dark, areas without coverage appear bright, areas with inadequate coverage appear gray. Users immediately reapply to bright spots, re-check to verify and proceed with genuine, confirmed protection instead of false confidence.
This works for three reasons. First, it overcomes sensory limitation by converting invisible UV patterns into visible light humans can perceive. For the first time cheaply, normal people who cannot afford to buy an expensive UV camera available can actually see whether sunscreen provides UV protection instead of guessing based on how lotion looks or feels. Second, it provides undeniable objective evidence that bypasses all cognitive biases. When you see your hand glowing bright white with gaps, you cannot rationalize it away, the visual proof forces belief change. Third, it provides specific, actionable feedback: "you missed between your fingers, around your knuckles, on your wrist". This specificity enables targeted correction.
The 100% adoption interest documented in this study proves that people WANT this technology once they understand the problem it solves. The challenge is not convincing people to use UV detection, the challenge is making them aware that they need it. Once awareness exists, demand follows immediately.
Real Impact
Consider a family heading to the beach. Parents carefully apply SPF 50 to their kids, believing they achieved good coverage (74% based on this study's data). They actually achieved 40%. After four hours in peak sun, the kids come home with burns on shoulders, ears, behind knees, between fingers, exactly the areas this study found everyone misses. The parents are confused: "But we were so careful!" They don't realize 60% of their kids skin was unprotected the entire time.
Now imagine the same family with UV verification. Apply sunscreen, check with phone's UV camera, see glowing white patches indicating gaps. "Oh! We missed behind the ears, between fingers." Reapply to those specific spots, check again, confirm complete coverage. This adds maybe five minutes to beach prep. After the same four hours, kids come home with no burns, genuine protection was achieved and verified. Over a summer with fifteen beach days, this prevents fifteen burn incidents. Over childhood, it prevents hundreds of burns and dramatically reduces lifetime cancer risk.
For outdoor workers spending 2,000 hours yearly in the sun, the impact compounds further. A construction worker who believes he achieves 74% coverage but actually gets 40% receives 60% unprotected exposure for 30 years equivalent to 7.3 years of continuous sun exposure or 2,700 beach days with no sunscreen at all. Outdoors workers have 3 times greater risk of skin cancer. With workplace UV verification as standard safety protocol (like hard hats), that same worker could achieve 80-90% coverage, reducing occupational UV exposure by 70-75%. Multiplied across 15 million outdoor workers, this could prevent thousands of melanomas annually.
Figure 11:
The Economic Reality
The Canada diagnoses 10,727 melanomas yearly as per 2025 melanoma Canada report, costing $25,000-$100,000 per case to treat, total economic burden exceeding $8 billion annually. If smartphone UV detection reaches just 10% of the population and improves average coverage from 40% to 65% (matching the 34-point perception gap documented in this study), epidemiological models suggest preventing 4,200-5,300 melanoma cases, saving $105-530 million in treatment costs. The implementation cost using $40 accessories would be $1.32 billion one-time, payback in 2.5-12.5 years, then ongoing savings forever.
Figure 12:
If manufacturers integrate UV sensors at $5-10 per phone during production, the cost to consumers becomes essentially zero (absorbed into phone prices). At 60% adoption (198 million people), this could prevent 25,000-32,000 cases annually, saving $630 million to $3.18 billion in treatment costs alone. Including non-melanoma skin cancers (5.4 million cases annually) and quality-of-life benefits, the total value is enormous. This may be one of the most cost-effective cancer prevention interventions available, requiring only that manufacturers implement the UV capability already proven to work in this study's prototype.
Although, this technology exist but it is very expensive, over the budget of normal people, but every single people has smartphone and by the integration of this technology could make the risk of melanoma less for millions of people and normal people could also use it. And this is the need of people due to the increase in skin cancer risks.
Figure 13:

From Laboratory to Global Market: The Commercial Viability of UV Sunscreen Verification
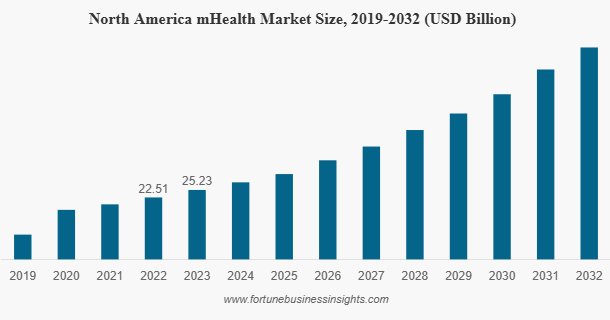
The mobile health industry known as mHealth, refers to the delivery of healthcare services and health monitoring through smartphones and mobile devices. According to Fortune Business Insights, the North American mHealth market was valued at $22.51 billion in 2022 and grew to $25.23 billion in 2023, with projections showing consistent and steep growth through 2032. This growth is driven by two forces that show no signs of reversing: the increasing penetration of smartphones across every demographic and income level worldwide and a growing consumer demand for personal health monitoring tools delivered through devices people already carry every single day.
Figure 14:
Mobile applications represent one of the largest segments within this market. People are no longer waiting for annual doctor visits to monitor their health, they are tracking heart rate, sleep quality, nutrition and dozens of other health metrics in real time through their phones. The market has proven repeatedly that when a meaningful health tool is made accessible through a smartphone, adoption follows at massive scale.
A smartphone-based UV sunscreen verification tool fits this market naturally and precisely. The consumer behavior shift toward mobile health has already happened. The infrastructure already exists. The devices are already in 6.8 billion hands worldwide. This project's findings, a 34 percentage point perception gap affecting 100% of people tested, combined with 100% adoption interest once the problem is revealed demonstrate that both the need and the demand are already there. The mHealth market does not need to be convinced that smartphone health tools are valuable. It has already proven that beyond any doubt.
The scale of this opportunity becomes even clearer when viewed through the lens of recent history. The COVID-19 pandemic fundamentally transformed how the entire world relates to mobile health technology. Governments deployed smartphone apps at unprecedented scale to protect public health, India's Aarogya Setu app reached over 150 million downloads, becoming one of the fastest adopted health applications in history. Canada launched its own COVID Alert app. Countries across Europe, Asia and North America built contact tracing, vaccination tracking and health monitoring tools delivered entirely through smartphone and the public used them. COVID did not just accelerate the mHealth market. It proved something far more important: when people understand that a smartphone app can protect their health, they adopt it immediately and at massive scale. The behavioral barrier that once existed between consumers and mobile health tools was permanently dismantled during the pandemic. That shift does not reverse. Those 150 million people who downloaded Aarogya Setu, those millions who used COVID Alert, those hundreds of millions who tracked symptoms and vaccination status through their phones, they proved that the world is ready for smartphone-delivered health protection. UV sunscreen verification is the next logical step in that same journey. The need is proven and market is primed. The world already knows how to use a health app to protect itself. This project provides the tool for the threat that was always there, silently causing cancer in one in 59 Canadian men, long before any pandemic made health apps headline news.
Figure 15:

Figure 16:

Conclusion
This project set out to answer one question: why do people who believe they are protected from the sun still develop melanoma at alarming rates? The hypothesis predicted that without UV feedback, people would fail to achieve accurate sunscreen coverage, because the human eye cannot detect ultraviolet wavelengths. The results did not just confirm this, they proved it with absolute consistency.
Every single participant, 100% without exception, overestimated their coverage. They believed they achieved 74% protection. UV imaging revealed the reality, 40% actual coverage. That 34-percentage-point perception gap is not a small error, it means people are absorbing nearly double the UV radiation they think they are, every single time they apply sunscreen, for their entire lives. This accumulated invisible exposure is precisely why people who "always wear sunscreen" still develop melanoma. They were never as protected as they believed.
What makes this finding so significant is its universality. The overestimation was not limited to uneducated individuals or uninformed participants. It occurred across every person tested, regardless of confidence, experience or carefulness during application. This proves the problem is not behavioral , it is biological. No amount of motivation, education or effort can allow a person to see wavelengths their eyes physically cannot detect. Fifty years of public health campaigns have failed not because people do not care, but because they have been trying to solve a sensory limitation with knowledge, and knowledge cannot overcome biology.
This is exactly why UV visualization succeeds where education fails. When participants saw their own hands glowing with unprotected gaps under UV light, gaps they had just confidently applied sunscreen over the reaction was immediate and visceral. No statistic, no warning, no educational video had ever created that moment of recognition. But seeing their own skin tell the truth did. Every single participant said they would use smartphone UV detection if it were available. Not most. Every one.
Although, technology is available and in the market but due to its high cost common people cannot afford it. The prototype that I built for this project, constructed from modified consumer hardware for under $60 proves this solution is not hypothetical. It works and is affordable. And through smartphone integration without any extra accessory like I made, and at a manufacturing cost of just $5-10 per device, it could reach billions of people worldwide, transforming UV verification from a specialized laboratory tool into something as ordinary as taking a photograph. The economic case is equally compelling: if UV detection reached 60% of the population and improved average coverage from 40% to just 65%, epidemiological models project 25,000 to 32,000 fewer melanoma cases annually, saving up to $3.18 billion in treatment costs every year.
The conclusion is clear. This is not a problem of knowledge on application of sunscreen. It is a problem of invisibility and this project proves we can solve it. We cannot educate our way out of a threat we cannot see. But we can build our way out of it. The technology exists. The need is universal, the demand is proven. What this project has demonstrated above all else is that the only thing standing between the current reality and a world with dramatically fewer melanoma cases is the decision to make the invisible finally visible.
Future Directions
This project answered its central question, but in doing so opened several new and compelling directions for future research, development and real-world implementation.
The most immediate and impactful next step is native smartphone integration. Manufacturers already include multiple camera modules in every flagship device UV detection would simply require removing the UV-blocking filter from one existing module and adding compact UV-LED illumination. A dedicated "UV Check" mode in the camera app would complete the implementation. At manufacturing scale, this addition would cost an estimated $5–10 per device probably, making it effectively free to consumers absorbed into phone pricing exactly the way fingerprint sensors, facial recognition and multiple camera systems became standard features over time. With 6.8 billion smartphone users worldwide, this single manufacturing decision could instantly democratize professional-grade UV verification for the entire global population. A companion app integrated into this hardware would automate coverage analysis using computer vision calculating exact coverage percentage, highlighting missed zones in color-coded overlays and providing specific audio or written guidance like "you missed between your fingers and around your left ear." This removes the need for users to interpret UV images themselves, making the tool accessible to everyone including children and elderly populations.
For the workplace, UV verification could become standard occupational health protocol similar to hard hat compliance with built-in smartphone UV cameras documenting daily sunscreen application for outdoor workers at the start of each shift. Given that outdoor workers face 2.5 to 3.5 times greater melanoma risk than indoor workers, this single intervention could prevent thousands of occupational cancer cases annually across construction, agriculture and landscaping industries.
Beyond the workplace, UV verification stations could be installed in public spaces where sun exposure is highest like beaches, outdoor pools, parks and sports facilities. Imagine a UV mirror station at the entrance of a beach, before stepping onto the sand, families and individuals check their sunscreen coverage under UV illumination, seeing exactly where they missed and correcting it on the spot before any damage begins. These stations could operate similarly to hand sanitizer dispensers free, publicly accessible and strategically placed where they are needed most. Schools could install them near outdoor entrances before recess. Ski resorts could place them at the base of hills. Stadiums could position them at gates. The technology required is simple and inexpensive and the impact would be immediate because as this study proved, people do not need convincing once they see their own gaps. They simply need the opportunity to see them.
Longer term, artificial intelligence integration could make the tool genuinely personalized. Machine learning models trained on thousands of UV images could learn each user's specific application habits, predict which areas they are likely to miss before they even check and track improvement over time. The app could evolve from a simple verification tool into a lifelong personal sun safety coach.
Beyond implementation, this project also opens several important new research questions worth investigating. The most natural follow-up experiment would be testing whether UV feedback improves coverage over time. This study proved people apply inadequately without UV imaging but a follow-up study could measure whether repeated use of UV verification trains people to apply better even without the tool. Do people internalize where they miss and self-correct after seeing their gaps multiple times? Or does the perception gap persist indefinitely without UV feedback every single time? This question has a massive implications for how the technology should be used in everyday life.
Another new question this study raises is whether the perception gap varies across different body regions. This project focused on hands a small, easily accessible area and the gaps documented here were already alarming. But what happens on the back, behind the ears, on the scalp or behind the knees, areas that are harder to see and reach? The perception gap on larger and less visible body parts could be dramatically worse than the 34 percentage points documented here, and a follow-up study using full-body UV imaging would reveal the true scale of the problem.
A further direction would be studying different age groups. All participants in this study were aged 16–20. Do younger children apply even less accurately? Do older adults perform better or worse? Does the perception gap shrink with age and experience or remain constant regardless further proving the biological rather than behavioral nature of the problem? It would also be worth studying how people emotionally and behaviorally respond to UV imaging over a longer period. This study captured the immediate reaction shock, recognition and an immediate desire to correct. But how do people feel a week later? A month later? Do they become more anxious about sun exposure or more confident because they now have a reliable tool? Do they share it with family and friends, creating a social ripple effect that accelerates adoption? Understanding these psychological responses would be critical for predicting real-world behavior once the technology reaches mainstream users.
The roadmap is clear. The technology is proven. The manufacturing pathway exists. Somewhere right now, someone is applying sunscreen before a day at the beach, believing they are protected, unaware that 60% of their skin is exposed. They are not careless, uneducated or uninformed. They are simply human, and humans cannot see ultraviolet light. This project exists because that should no longer be an excuse. The invisible can be made visible. The question is no longer whether we can do it. The question is whether we will.
Citations
-
Branstrom, R., Kristjansson, S., & Ullen, H. (2006). Risk perception, optimistic bias, and readiness to change sun related behaviour. European Journal of Public Health, 16(5), 492–497. https://doi.org/10.1093/eurpub/cki193
-
Canadian Cancer Society. (2024). Canadian cancer statistics: A 2024 special report on the economic impact of cancer in Canada. Canadian Cancer Society. https://cancer.ca/en/about-us/media-releases/2024/cancer-statistics-special-report
- Canadian Cancer Society. (2024). New report released by the Canadian Cancer Society reveals that cancer costs the average patient nearly $33,000 in their lifetime. https://cancer.ca/en/about-us/media-releases/2024/cancer-statistics-special-report
- Cowern, D. [Physics Girl]. (2017). Sunscreen in UV [Video]. YouTube. https://youtu.be/V9K6gjR07Po
- Emergen Research. (2025). mHealth solution market size, share & trends analysis, 2024–2034. Emergen Research. https://www.emergenresearch.com/industry-report/mhealth-solution-market
- Fortune Business Insights. (n.d.). Health and wellness market size, share & industry analysis. Fortune Business Insights. https://www.fortunebusinessinsights.com/health-and-wellness-market-110596
- Geist, M. (2020, August 2). Why I installed the COVID Alert app. Michael Geist. https://www.michaelgeist.ca/2020/08/why-i-installed-the-covid-alert-app/
- Government of Canada. (n.d.). Skin cancer and sun safety. Public Health Agency of Canada. https://www.canada.ca/en/public-health/services/sun-safety/skin-cancer.html
- Harvard Health Publishing. (n.d.). Sun poisoning: Symptoms and signs you've had too much sun. Harvard Health Publishing. https://www.health.harvard.edu/digital_first_content/sun-poisoning-symptoms-signs-youve-had-too-much-sun
- Isnawati, M., Adriani, M., & Mahmudiono, T. (2022). Behavior of sunscreen usage among medical students. Journal of Public Health Research, 11(2), 1–6. https://doi.org/10.4081/jphr.2022.2691
- JSAUX. (n.d.). 2 pack USB C to USB adapter, type C to USB 3.0 OTG cable [Product listing]. Amazon Canada. https://www.amazon.ca/dp/B07BS8SRWH
- Kamas. (n.d.). Harlica tools ZWB2 ultraviolet UV band pass filter UV flashlight diameter 28mm thickness 2mm [Product listing]. Amazon Canada. https://www.amazon.ca/dp/B07N41VSBL
- Keenso. (n.d.). OV2643 USB camera module autofocus mini camera board 2MP 120° wide angle camera module with OV2643 chip [Product listing]. Amazon Canada. https://www.amazon.ca/dp/B07QGZCF8N
- Manca, A., & Ciani, O. (2021). Distinguishing features in the assessment of mHealth apps. Expert Review of Pharmacoeconomics & Outcomes Research, 21(4), 521–526. https://doi.org/10.1080/14737167.2021.1891883
- Melanoma Canada. (n.d.). Stats and facts. Melanoma Canada. https://melanomacanada.ca/understanding-skin-cancer/melanoma/stats-and-facts/
- MidOpt. (n.d.). BP324 near-UV bandpass filter to block visible & infrared light. Midwest Optical Systems. https://midopt.com/filters/bp324/
- Muller, D. [Veritasium]. (2017). What if you could only see the world in UV? [Video]. YouTube. https://youtu.be/GRD-xvlhGMc
- Nickerson, R. S. (1998). Confirmation bias: A ubiquitous phenomenon in many guises. Review of General Psychology, 2(2), 175–220. https://pages.ucsd.edu/~mckenzie/nickersonConfirmationBias.pdf
- Occupational Cancer Research Centre. (2018, October 16). Outdoor workers have 3 times greater risk of skin cancer. Occupational Cancer Research Centre. https://www.occupationalcancer.ca/outdoor-workers-have-3-times-greater-risk-of-skin-cancer/
- Project 326. (2025, September 26). Tiny night vision camera project [DIY] [Video]. YouTube. https://www.youtube.com/watch?v=GRD-xvlhGMc
- Sharot, T. (2011). The optimism bias. Current Biology, 21(23), R941–R945. https://www.sciencedirect.com/science/article/pii/S0960982211011912
- Sony Semiconductor Solutions Group. (n.d.). Ultraviolet (UV) image sensor technology. Sony Semiconductor Solutions Group. https://www.sony-semicon.com/en/technology/industry/uv.html
- Team MyGov. (2020, July 3). Aarogya Setu: Transcending digital health care. MyGov Blog, Government of India. https://blog.mygov.in/aarogya-setu-transcending-digital-health-care/
Acknowledgement
I would like to acknowledge my Parents, for their constant support and encouragement throughout this journey. I would also like to thank my uncle, Mr. Parth Pandya a Software Engineer at Texas Instruments, for his technical guidance and helping me understand the principles behind UV detection and imaging. I would like to thank my teacher, Ms. Malhi for providing valuable feedback and answering all of my questions regarding this project. Lastly, I would like to thank all the individuals who took the time to participate in my experiment, as their responses were greatly appreciated and essential to this project.