Coagulation Factor & Hemophilia
Grade 7
Presentation
Problem
Hemophilia treatments have some problems that make them less dependable for patients. One big issue is that these treatments don't work the same for everyone because of things like genetics and immune responses. The usual way of getting treatments through frequent infusions can be hard for people to follow and disrupt their daily routines. Some patients also develop inhibitors, which are like blockers that stop the treatment from working well. The advanced treatments are not easy to access for everyone and can be expensive, making it harder for some people to get the care they need. To make hemophilia treatments more reliable, we need simpler and easier options that consider these challenges, so everyone can get consistent and effective help.
Method
The following text is the method of applying gene therapy:
1. AAV preparation:
Scientists use the AAV containing a functional gene. This gene acts as a blueprint for the production of the missing clotting factor in individuals with hemophilia.
2. AAV:
The gene is inserted into AAV virus. This vector is like a delivery vehicle, helping transport the gene to the target cells in the body.
3. Infusion:
Doctors introduce the medicine into the patient's body using a process called intravenous (IV) infusion. This involves injecting the medicine directly into the bloodstream through a vein, usually in the arm.
4. IV Infusion Details:
The administration is done through a small tube or catheter, known as an IV line. This is a common medical procedure, similar to how some medications are delivered in a hospital.
5. Duration of Infusion:
The IV infusion process can takes 1-2 hours. The exact duration depends on the specific treatment protocol and individual circumstances. In some cases, patients may undergo multiple sessions over a few days.
6. Clotting Factor Production:
Modified cells begin producing the missing clotting factor, giving the body ability to form blood clots.
7. Monitoring Progress:
Doctors closely monitor patients during and after the procedure. They assess clotting factor levels and overall well-being, ensuring the therapy is effective and safe over the long term.
Research
What is coagulation?
Usually every time you have a cut or bruise your blood clots to stop the bleeding. Clotting is a complex process and there are 4 main components that make it possible; platelets or cell fragments, clotting factor (also known as special proteins), fibrin (protein mesh), and finally, other cells (e.g.,Red and white blood cells). Because cloth formation is so important, platelets and clotting factors are always available; floating around in your blood.
4 steps to coagulation
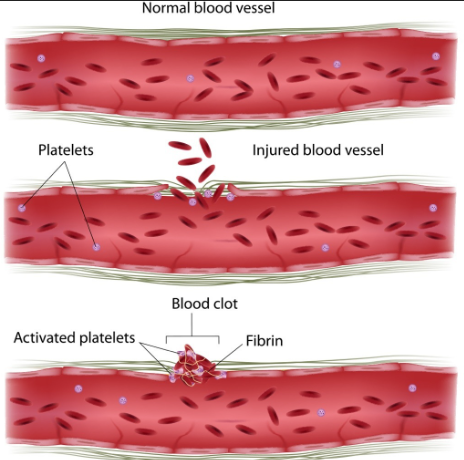
When there is a tear in a blood vessel, the first thing that happens is that the nearby platelets are activated, and become sticky. They start sticking to each other and to the sides of the hole, usually the platelets can form a temporary plug but this plug isn't strong enough to hold for too long, so it must be reinforced.
Passing by clotting factors turn themselves on or activate and add themselves to the platelets plug. A special kind of clotting factor can weave itself together with others of the same kind and form a web of fibrous tissue called fibrin this acts as a glue. Other cells like red and white blood cells can also help reinforce the clot and help it become stronger.
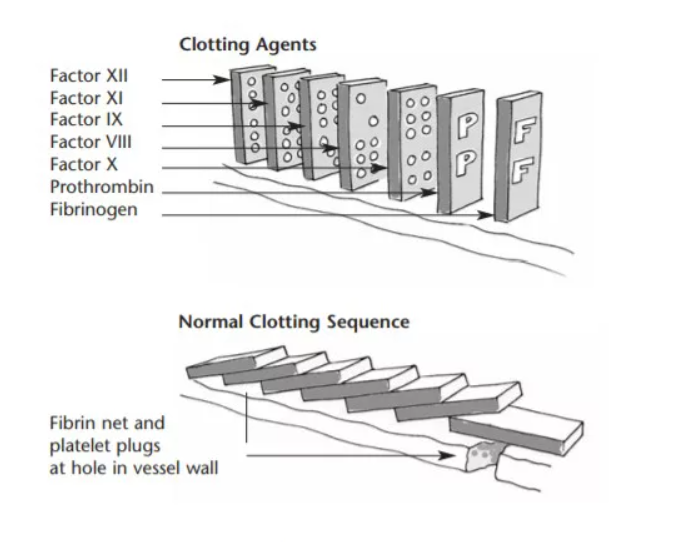
Coagulation Cascade
When a blood vessel is damaged, there are four stages in the normal formation of a clot.
Stage 1: The blood vessels are damaged and the bleedings starts.
Stage 2: The blood vessels constrict to slow the flow of blood to the injured area.
Stage 3: Platelets stick to, and spread on, the walls of damaged blood vessels. This is called platelet adhesion. These spreading platelets release substances that activate other nearby platelets which clump at the site of injury to form a platelet plug. This called platelet aggregation.
Stage 4: The surface of these activated platelets then provides a site for blood clotting to occur. Clotting proteins like factor VIII and IX circulating in the blood are activated on the surface of the platelets to form a mesh-like fibrin clot.
These proteins (factors I, II, V, VII, VIII, IX, X, XI, XII, XIII and von Willebrand factor) work like dominos, in a chain reaction. This is called the coagulation cascade.
Understanding Coagulation with an Experiment
Materials:
- Red Sodium Alginate (10ml)
- White Sodium Alginate (1.2ml)
- Calcium chloride (⅛ tsp/600mg)
- Pipette
- Cup
- Water (50ml)
- Stir stick
- Vial - Optional
Procedure:
- Fill your cup with 50ml of water and add 600mg of calcium chloride and stir until the powder is dissolved.
- In a separate bowl, squeeze 10 ml of Sodium Alginate. Grab a pipette and gently srop blobs of sodium Alginate into the Calcium chloride bowl. Red Blood cells start forming, Repeat until empty.
- Drop 6 drops of white Sodium Alginate into a spoon and hold the spoon in the Calcium chloride mixture for 10 seconds. A white blood Cell is formed. Repeat thrice.
- Drain the water and scoop the red and white blood cells and place them into an empty vial.


Coagulation in Human Body vs Experiment
|
In the Human Body |
What I used in the experiment |
|
|
Substance that requires Coagulation |
Blood |
Sodium Alginate Solution |
|
Source of Calcium for Coagulation |
Platelets and Factors (factors I, II, V, VII, VIII, IX, X, XI, XII, XIII and von Willebrand factor) |
Calcium Chloride Solution |
|
End Product |
Blood Clot |
Semi-Solid balls of Calcium Alginate |
Experiment explanation
In the experiment we displayed how coagulation works to make a semi-solid seal, or in the experiments case, a semi-solid ball. In the experiment we used sodium alginate as the substitute for blood since both clot. The thing that makes the blood clot is the platelets and factors (factors I, II, V, VII, VIII, IX, X, XI, XII, XIII and von Willebrand factor)and in the experiment its calcium chloride solution. The main goal of the experiment was to learn and observe the clotting process first hand.
Observation & Analysis of experiment
Observation: As far as I could see the sodium alginate took a matter of seconds to form the semi-solid ball, though I did notice when using the spoon that the bigger the clump of sodium alginate the longer you need to keep it submerged before it becomes stable, but the entire procedure of making a ball took about 10 seconds.
Analysis: This was a fun and creative way of displaying coagulation, and showing red and white blood cells with white and red sodium alginate. By using a spoon or pipet you can also make some cool shapes and stuff which gives you some creative freedom. The experiment was a good way to show how a liquid like blood or sodium alginate can clot in a matter of seconds, and a good hand-on experience to help understand the basic principles of coagulation.
What is hemophilia?
Hemophilia is a genetic bleeding disorder where the blood doesn't clot properly. This can result in spontaneous bleeding or excessive bleeding after injuries or surgeries. Clotting factors, proteins in the blood, usually help stop bleeding. Individuals with hemophilia have low levels of either factor VIII (8) or factor IX (9). The lack of a clotting mechanism means that injuries, like cuts and abrasions, may bleed for longer than would be expected. The main danger to hemophilia, however, is internal bleeding that may occur. In this instance, the blood can pool in joints and organs, triggering an immune response that damages the affected area.The severity of hemophilia is determined by the amount of these factors in the blood. The lower the factor level, the higher the risk of bleeding, leading to potential health issues.
Although over 200 000 men have hemophilia, only 25% of them are actually diagnosed. In fact, in most third-world countries, there is little to no awareness of such conditions, and most people with hemophilia can't access the proper medication. Here in Canada, a first-world country, you can receive prophylaxis, the best treatment for hemophilia as it helps prevent bleeding. As of now, there is no way to permanently eliminate the condition since it's genetically passed down, but prophylaxis do make it possible to live a normal life even with hemophilia. However, the fact that third and second-world countries don't really have proper medication still remains. Scientists are trying to find solutions but haven't made too much progress, as most solutions either cost too much, are dangerous, or too time-consuming.
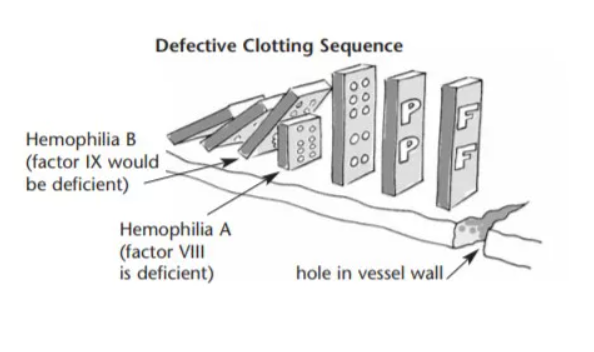
Coagulation Cascade with Hemophilia
When one of the proteins, for example, factor VIII, is absent, the dominos stop falling, and the chain reaction is broken. Clotting does not happen, or it happens much more slowly than normal. The platelets at the site of the injury do not mesh into place to form a permanent clot. The clot is ‘soft’ and easily displaced. Without treatment, bleeding will continue until the pressure outside the broken vessel is equal to the pressure inside. This can take days and sometimes weeks.
How hemophilia passed through generations
Hemophilia almost always pases through genes. Genes are basically the blueprints to you, they contain the informations on how to make you, from the color of your eyes to the speed your fingernails grow at. These genes are inside chromosomes which are inside the cells in your body, there are 46 chromosomes in each cell of your body, 23 from your mother and 23 from your father. These chromosomes are called X and Y chromosomes.
In hemophilia there is a defective X chromosome, this chromosome is not able to produce either no factors XIII at all or very little amounts of it. Now males have X and Y chromosomes while females have 2 X chromosomes. When a male and a female have a child either one of the Xs of the mother gets passed and either the X or the Y gets passed from the father. If the X gets transferred then its a girl and if the Y gets transferred then its a boy.
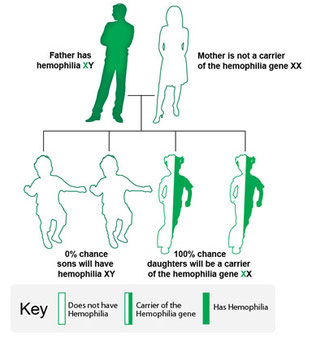
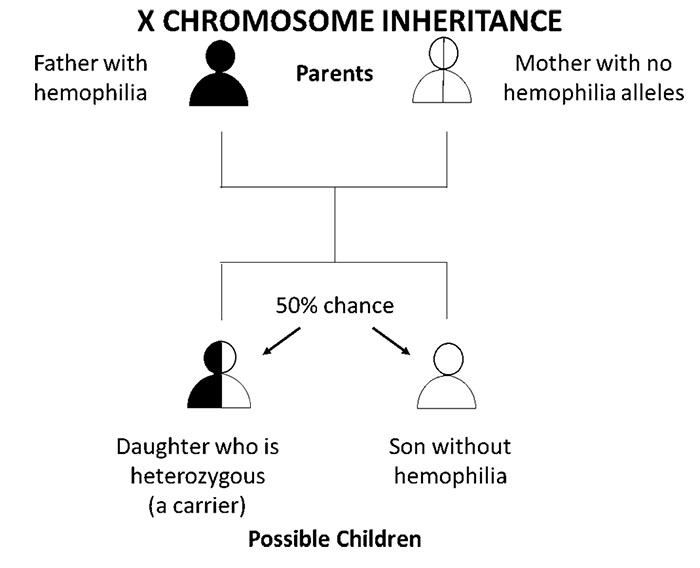
Now if the father has hemophilia this means his X chromosome is defected in this case if they have a boy there is absolutely no chance that the son will have hemophilia since for him to be a boy he needs a Y chromosome and since only the X is defected he doesn't end up with hemophilia.
On the other hand if its a girl then she will no matter what have hemophilia since to be a girl she needs 1 X from her mother and the other from her father and since the X from her father is defected she has hemophilia, though she does not have full hemophilia and is only a heterozygous or a carrier since in the female body there is 2 X’s and if one X does not function properly the other can partially do what the other is missing. This can lead to minor symptoms like excessive bleeding and longer clotting time but overall it's not that effective on females. And because hemophilia doesn't affect females all that much it can stay silent for generations and not get noticed until it gets transferred to a male.
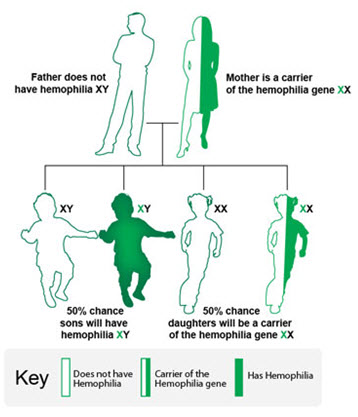
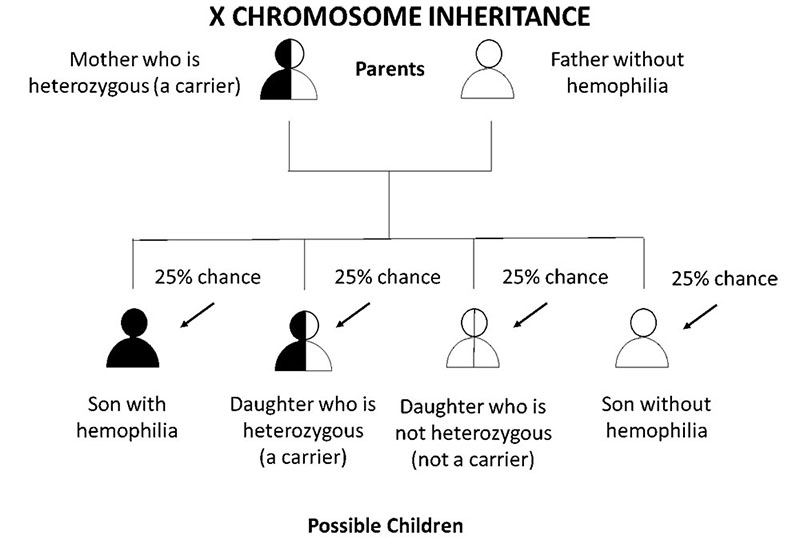
If the mother is a heterozygous her children have a 25% chance of getting it, if its a girl she can get either one of her mothers X’s and has a 50% chance of getting it, and the same goes for the boy he can get either one of the mothers X’s since neither is obligatory for him to get.
Symptoms
Often the first signs of hemophilia in babies is excessive tooth bleeding and constant bruises. As babies learn to crawl and walk they fall quite often leading to many scratches and bruises, though this is common in babies, hemophiliacs will get them more easily and more often. Internal bleeding is unlikely until the age of 2. Other symptoms in youth and adults are:
- Joint bleeding (knees, elbows, ankles, shoulders, hips, and wrists)
- Mouth bleeding (cut, bitten tongue, and loss of tooth)
- Bleeding in soft tissue and muscles
- Surface bruising
- Hematuria (blood in urine)
It is also possible to get bleeding in vital areas which can be very harmful, and lead to serious pain and injuries.
Diagnosing hemophilia
If a doctor suspects a person has hemophilia they will conduct a blood test. He or she will do some simple blood tests to measure the amount of factor VIII and IX in the patient's body. If they are lacking factor VIII they have hemophilia A and if they lack factor IX then they have hemophilia B. The tests will also tell the doctor how severe the hemophilia is, if they lack less than 1% of the average levels then they have severe hemophilia, f its 1-5% of the average levels then he or she has got moderate hemophilia and if it's 5-30% then the hemophilia is very mild. These tests will usually be returned in 1-2 weeks.
Current Treatments
Basic treatments:
There are 2 basic treatments to hemophilia and unfortunately both of the are not permanent, in fact the effects of these will on last 2-3 days. The first 1 is straight up plasma which is extracted from human blood. Plasma contains all the components needed to clot, including factor VIII and IX. But since the liver is really good at recognizing intruders it flushes the unused parts and you need to get another dose. The same goes for recombinants, which are genetically engineered cell line made of DNA technology. Recombinants also stick around for 2-3 days and get flushed out by the liver. The 2 main differences in these 2 are 1 the fact that recombinants contain only VIII/IX and plasma contains all the factors and everything else the 2nd difference is that plasma is from actual human blood for which we need donors all the time while recombinants are lab created and are overall more effective and easier to produce. This treatment method of Recombinants is called prophylaxis.
When the person gets injected there blood has the normal amounts of the factor there missing as the day goes on, there factor levels decrease more and more, and eventually there body runs out. As of now he median half-life of factor VIII is 16-18 hours; factor IX 50-100 hours.
Specific medications
For hemophilia A, standard half-life products are used such as Kovaltry, Nuwiq, Xyntha and Zonovate. The extended half-life products are, Eloctate, Esperoct and Jivi. As for the hemophiliacs who have been previously treated and have a risk of development of inhibitors and or patients whose bodies have created antibodies to factor VIII plasma works better. On the other hand patients who have hemophilia B standard half-life products are Benefix and Rixubis and the extended half-life products are Alprolix, Idelvion and Rebinyn. And again hemophiliacs who need plasma get it from the brand Immunine.
History of Hemophilia
First documentation
Hemophilia was documented in 1828 by Dr. Scholien and his student Friedrich hopff at the university of Zurich. It was originally named haemorrhaphilia but was later simplified to hemophilia. But there had been many more documentations of hemophilia even before 1828.
The first known documentations of excessive or abnormal bleeding were in 2nd century AD written in the Talmud, Jewish rabbinical writings which informed of religious and traditional laws. These laws allowed male infants to avoid circumcision if 2 of their brothers had previously died due to hemorrhage following the procedure. An arab physician named Abu Khasim in the 10th century mentioned that male member within certain families died after traumatic events due to excessive bleeding.
The royal disease
Hemophilia is often referred to as the “royal disease” since it often appeared in royal families of England, Russia, Spain, and Germany in the 19th and 20th centuries. Queen Victoria is now known to be a carrier of hemophilia and passed it down to 3 out of her 9 children. 1 out of the 3 children, Prince Leopold Albert, died at the age of 30 due to excessive bleeding after falling. Her daughter, Princess Alice Mary, passed the condition to her daughter, Princess Alix Beatrix, who married Tsar Nicholas of Russia. They had a son, Alexei Nikolaevich, whom had inherited hemophilia from his mother. This caused Nicholas to hire a siberian monk named Grigori Rasputin, as a healer for his son. Rasputin become a close confident of NIcholas and was able to influence the decisions of the royal family. This led to a widespread of rumors and accusations of corruption by the locals, which further betrayed the public's trust in the monarchy. Rasputin was murdered in 1816 and the collapse of the russian empire were some of the events leading up to the russian revolution. Princess Beatrix Feodore was Queen Victoria's youngest child and the 3rd child to have received the defective gene, she passed it down to several of her children, for 3 generations after Queen Victoria, hemophilia was seen in various different european royal families in which her children/ grandchildren had married into, but eventually the condition did die out.
Discovering hemophilia
In 1803 a physician named John Condrat Otto published a article about a hemorrhagic bleeding disorder that ran through certain family trees and only seemed to affect men, he then went on to trace back all the affected families and found that they all carried a common female ancestor back in 1720. In a paper published in 1813 John Hay suggested that men who have the trade might pass it down to their unaffected daughters. Gregor Mendel made the discovery of genetic inheritance, and though it was not directly related to hemophilia it did spark the research on genetic transmissions of disease which later prompted the later understanding of rare X-linked inheritance which is how hemophilia gets transferred. From 1920-1960 researchers started identifying clotting factor deficiency caused by gene mutations. In 1947, a doctor named Alfredo Pavlovsky in Buenos Aires, Argentina, uncovered hemophilia types A and B. He figured out the difference between them by mixing blood from a hemophilia type A patient with that of a type B patient. This experiment showed that the clotting time improved.
Case study
I’ve always seen my dad putting some injection into his arm once or twice a week and my mother helped him do that. Eventually I found out he has some blood condition and not only him, I was also carrier of that condition. That made me so curious to learn about what exactly it was and how I got the same condition as my dad.
I interviewed my Grandma for this project and this is what she told me about my dad.
“Before he was diagnosed with hemophilia at the age of five, he endured constant joint pain in his left knee. Living in a small town of Pakistan at that time, the concept of such a condition wasn't heard of. I took him to many doctors and clinics to get medications for his joint pains, easy bruising, and swelling. Unfortunately, the medical professionals in the small town were unfamiliar with this rare condition. They gave their opinions and gave many medications such as anti-inflammatories, painkillers, and drugs for arthritis. However, none of these treatments were effective, they caused additional issues like rashes and acne.
When he was 5, he fell and got an injury that didn't stop bleeding for two days. It made him weak because he lost a bunch of blood. We took him to the hospital, but they couldn't figure out what was wrong, so they suggested us to take him to a specialist in Lahore. (Lahore is the 2nd largest city of Pakistan and had a lot better medical facilities and hospitals). After some tests, they found out that he had hemophilia. They treated him with Plasma extracted from blood. Then I had to go to Lahore 3 to 4 times a month to get plasma treatment and every time finding blood donors was so hard. His pains were better and he complained a lot less about his joints after. We came to canada when he was about 9. Here doctors tested him and discovered that he has the severe case where his Factor VIII levels are 0. They put him on prophylaxis.”
Before my parents had me, Hemophilia doctor at Foothills hospital Dr.Poon explained them that all the daughters of my dad are going to be carriers of Hemophilia. Now I’m aware of the fact that I’m the Hemophilia carrier and I could pass this to my next generations.
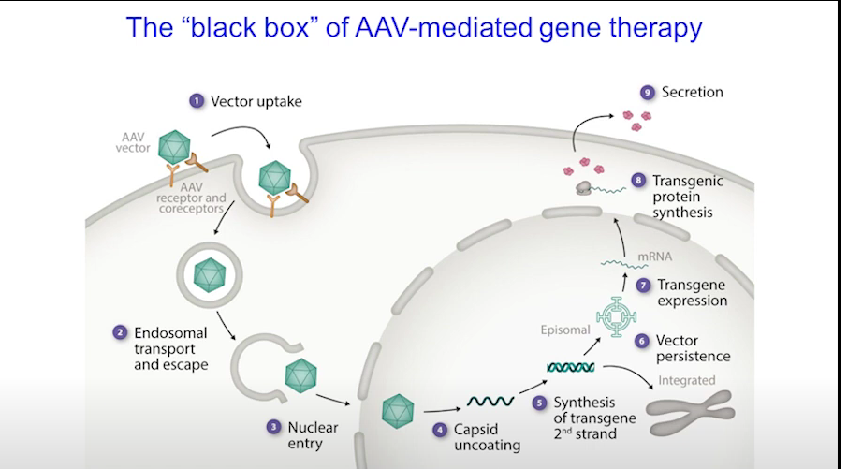
Gene therapy
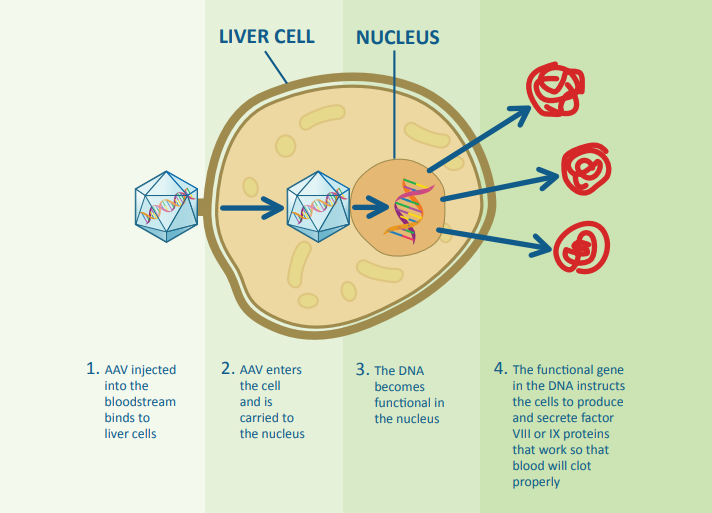
Gene therapies for hemophilia currently in trials and recently approved use a modified virus called adeno-associated virus (AAV) to transfer the gene responsible for producing factor VIII or factor IX into the liver cells (hepatocytes). The AAV is good at entering these cells without causing the diseases typically associated with the virus.
After a one-time intravenous (IV) infusion, similar to receiving clotting factor, patients can start making their own factor VIII or IX. However, because the body's immune system develops antibodies to AAV after the infusion, this treatment can't be done a second time
Gene therapies for hemophilia currently in trials and recently approved use a modified virus called adeno-associated virus (AAV) to transfer the gene responsible for producing factor VIII or factor IX into the liver cells (hepatocytes). The AAV is good at entering these cells without causing the diseases typically associated with the virus. After a one-time intravenous (IV) infusion, similar to receiving clotting factor, patients can start making their own factor VIII or IX. However, because the body's immune system develops antibodies to AAV after the infusion, this treatment can't be done a second time.
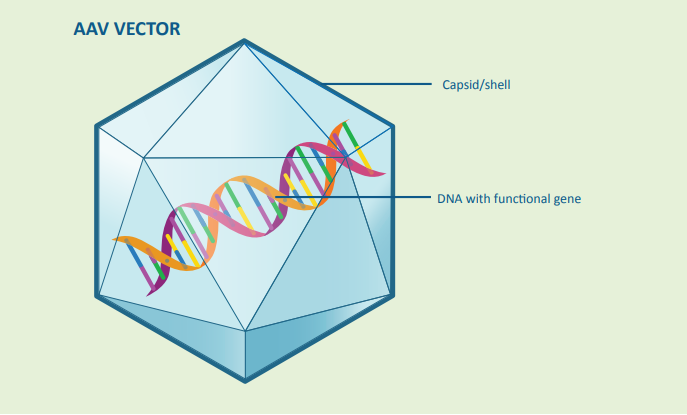
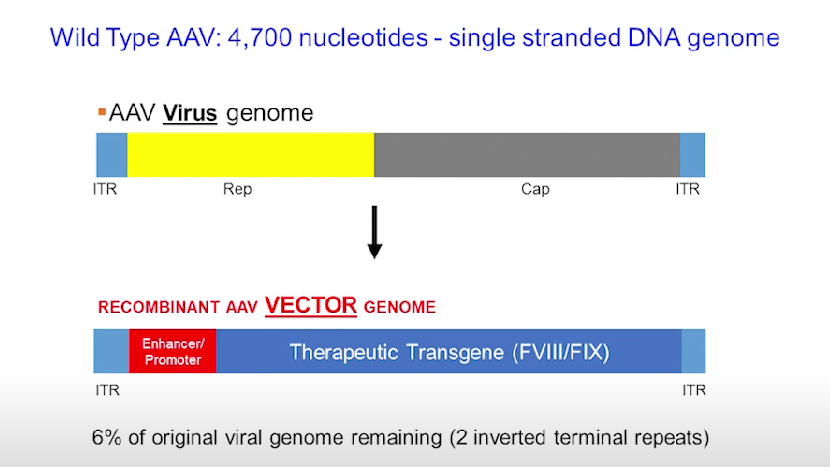
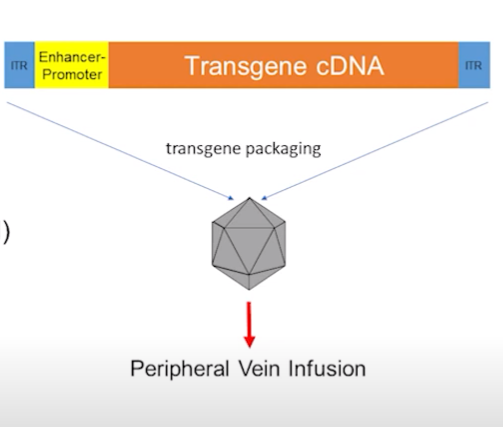
AAV or Adeno associated virus is the vector that we use to send the modified genes through. A AAV has a genome which is encapsulated in just one chromosome inside this chromosome there is 2 genes, (the human body has 46 chromosomes and 20 000 genes) these genes are called “Rep” and “Cap” which are the yellow and gray bars. Recombinant AAV vector genome is created by replacing the 2 genes with factor VIII/IX on one end there is a enhancer which is a regulatory element to make the genes continue creating the protein. Then on either side there is the ITR which is the outlining and protects the genes. This vector is packaged into a protein called Capsid shown in the image ready for peripheral vein infusion.
Once transmitted into the body, these vectors have tendency to go to the liver and that's exactly where it reaches and comes out of its capsid and somehow commands to make required Protein which secrets into the bloodstream and that's how our goal is achieved.
Information collected from Hemophilia gene therapy; dream or reality podcast Nov 2023:
- 40% of hemophilia B patients and 60% of hemophilia A are not eligible, these include:
- Under 18 (98% of the vector does not get dissolved into the chromosome and stays in structures called episomes which gets lost when the cell divides: the kids liver is still developing so it will be lost by the time they get older)
- Those who have moderate or mild hemophilia
- Those with liver problems
- Those who are immune to AAV
- Those who have or had inhibitors
- Hypertoxicity may be caused because of gene therapy- about 2-4 months after infusion.
- Factor IX therapy is more effective than factor VII because the cells we are injecting the vector specialize in creating factor IX (they can create factor VII but they won't be as good as the naturally produced ones)
- Absolutely irreversible treatment-no matter out come
- Once infusion done you must often visit clinics to get regular check up and blood tests to check liver toxicities, liver enzymes, and factor levels in your blood.
- You might need occasional proflaxys and maybe need to go completely back to prophalys in the future.
- Starts working after 2-4 weeks.
- 5% have absolutely no response to gene therapy
- Outcomes may vary on person to person
- What we don't know:
- Long term risks
- Immune response
- Why the factor levels may decline over time
- Rare toxicities
- If you can get cancer because of it
- Shared decision making
- Normal people have both clotting factors and anti-clotting factors, if someone has less clotting factors they may go back to normal if you decrease the anti-clotting factors.
Observations
- Prophylaxis Challenges:
- Effectiveness: Prophylaxis works but needs frequent infusions several times a week.
- Quality of Life: It makes life better, but it's expensive and not easily available, especially in countries like India where most number of hemophilia patients are reported. Also, sticking to the treatment schedule is hard.
- Gene Therapy Insights:
- Procedure: Gene therapy involves a one-time infusion of a special virus for continuous clotting factor production in the liver.
- Cost Effective: Gene therapy costs are different from regular treatments and can be more cost-effective. It's all in one treatment.
- Implementation Challenges for Gene Therapy:
- Complexity: Gene therapy is complicated and needs careful administration and monitoring.
- Limited Centers: Only a few Canadian centers can do gene therapy, especially in smaller places.
- Patient Eligibility and Monitoring:
- Limited Interest: Only a small number of patients might want or qualify for gene therapy at first.
- Monitoring Importance: Checking for reactions is really important, and it involves frequent tests, longer time period to observe the reactions or side effects and quick action plan if something's wrong.
Analysis
- Prophylaxis vs. Gene Therapy:
- Prophylaxis Strengths: It works but has problems with cost and sticking to the plan.
- Gene Therapy Potential: It's a big deal because it's a one-time thing, might cost less, and could cure the problem.
- Implementation Challenges:
- Resources: Not many places can do gene therapy at first, and not everyone knows how.
- Monitoring Complexity: Watching for problems is crucial, and it can be tough in places that don't have much experience, definitely needs a lot more research and testing before it could be implemented with confidence.
Data
(Since my project is a research project I do not have any data to write)
Conclusion
*JAN 3, 2024
“Pfizer Canada ULC announced that Health Canada approved an Adeno-associated viral (AAV) vector based gene therapy for the treatment of adults age 18 years or older with moderately severe to severe hemophilia B (Factor IX deficiency) who are negative for neutralizing antibodies to variants serotype Rh 74” www.newswire.ca
Gene therapy for hemophilia is definitely real but still has some fixing to do. It's a one-time treatment, but regular check-ups are needed. Results vary, and 5% may not even respond. We're uncertain about long-term risks, immune reactions, Cancer risks, and why factor levels might drop over time. Eligibility is limited, and there's a risk of issues in the first few months. As of Jan 3rd, 2024 gene therapy has been approved for Hemophilia B with some conditions but we still have long way to go for a successful implementation of this treatment for hemophilia A and for broader spectrum of patients.
Citations
- www.cdc.gov/ncbddd/hemophilia/inheritance-pattern.html
- Rarediseaseadvisor.com
- Gene therapy for hemophilia may soon become a reality — but when? | Healthing.ca
- All-About-Hemophilia-Gene-Therapy.pdf
- Gene therapy for hemophilia: an imperative to succeed - HOUGH - 2005 - Journal of Thrombosis and Haemostasis - Wiley Online Library
- https://youtube.com/playlist?list=PLGmdqy_hGQx3f9WA11RSOnCm5DvZ5PSok&si=0f7kDpFF1Wb_bahR
- www.newswire.ca
- Hemophilia.ca
- Youtube.com
- Sciencebuddys.org
- (PDF) HEMOPHILIA GENETICS DIAGNOSIS AND TREATMENT (researchgate.net)
- https:///clotting-problem-in-hemophilia/
- Google.com
Acknowledgement
The following people helped me through out my research and I would like to thank them for there contributions:
Kiran Riaz (my mother)
Jyoti Nambiar (my science teacher)
Fatima Iqbal
Zahid hussain (my father )
Namazan Pir (my grandmother)