10 people, 1 body
Chloe Fabiyi
Calgary Girls Charter School
Grade 9
Presentation
No video provided
Problem
Dissociative Identity Disorder (DID) is an extreme form of PTSD that has devastating effects on patients. DID has degenerative effects on the central nervous system (CNS), and common symptoms/side effects include inter-identity amnesia, non-epileptic seizures, major psychobiological differences between TIS (traumatic identity states), co-morbid depression/PTSD, suicide attempts, and self-harm behaviours. Not only does it have debilitating effects on the body, but it is also highly stigmatized in the general public, and even many mental health professionals don't believe in the validity of DID as a post-traumatic disorder. The condition is under researched, the average patient spends 12 years inpatient before the proper diagnoses is made, many patients are misdagnosed with bipolar disorder (BD), borderline personality disorder (BPD), depression, and schizophrenia, the disorder effects functioning to the point that some are unable to work, form deep connections, and fully enjoy leisure, and it has high rates of lonliness/isolation, with many patients feeling as if not only do the general public and mental health professionals not understand them, but that they don’t understand themselves. The current treatment for DID is long-term weekly psychotherapy with the hope of merging all alters into one, but that doesn’t factor in all psychological symptoms, neurologic changes, and biological changes. This project researches what DID is, how traumatic history affects the development/presentation of DID, and neurological changes seen as a result of DID in comparison to controls. Using this information, an intensive treatment plan for DID, factoring in psychological symptoms, neurologic changes, and psychobiological factors, will be made.
Method
To answer the question of what DID is from a psychological, biological and neurologic perspective to create a treatment plan factoring these things, research on the following was done; the development of DID, the effects of DID on peoples lives, what EPs/TIS’s are, how many alters the average person has, the different types of alters/how those alters develop relative to traumatic history, case studies to compare the experiences of those with DID, changes in the neuroanatomy in those with DID compared to controls, how the negative affects on the CNS/psychobiological symptoms come to be, how to fight against the negative affects on the CNS/psychological symptoms, and how/why potential treatment plans could work. Using all this information, a list of all relevant research was put together. Using that research, a potential treatment plan looking at multiple individual factors for maximum effectiveness was put together. It is hypothesised that traumatic history will change the presentation/development of DID, since it’s a post-traumatic disorder. As with other post-traumatic disorders, such as PTSD, changes in triggers and symptoms depending on traumatic history are observed, so it is hypothesised that this trend will continue with DID. It is hypothesised that differences in types of alters, frequency/cause of switching, and symptoms of DID will be observed. It is hypothesised that DID will change the brain anatomy, specifically having a negative correlation with the limbic system and frontal lobe of the brain relative to healthy controls and controls with BD, BPD, schizophrenia, and depression. This is hypothesised because the limbic system is the “emotional centre” of the brain, which is responsible for our memory and emotional regulation, and DID has a serious effect on memory and emotional regulation. The frontal lobe is responsible for the formation of personality, something that is impaired with DID It is hypothesised that there will be changes in the biopsychology and the neuropsychology between TIS. It is hypothesised that there will specifically be changes in the blood pressure, heart rate, aroused neurons/brain areas, and blood flow. It is hypothesised that there will be a higher heart rate, blood pressure, and a flight/fight reaction in protective TIS when presenting, because protective alters come out when a threat is sensed, so even if there isn’t a life/death situation, they will act in such a way. It is hypothesised that there will be hyper arousal in the hippocampus and amygdala when protective alters present because that is where the fight/flight response is seen in the brain. It is hypothesised that non-epileptic seizures seen in DID will be a result of unresolved trauma/stress presenting a physical way, and possible treatments may include stress management.
Research
What is DID?
- Dissociative identity disorder (DID) is a mental health condition where you have two or more separate personalities that control your behavior at different times. When personalities switch, you’ll have gaps in your memory (1)
- Different identities or alters tend to have different interests, abilities and skills, personalities, behaviours, memories and though patterns
- Theyre each like there own people, with their own ethnicities, ages, skills, ect.
- DID reflects a failure to integrate various aspects of identity, memory, and consciousness into a single multidimensional self. Usually, a primary identity carries the individual's given name and is passive, dependent, guilty, and depressed. When in control, each personality state, or alter, may be experienced as if it has a distinct history, self-image, and identity. The alters' characteristics—including name, reported age and gender, vocabulary, general knowledge, and predominant mood—contrast with those of the primary identity. Certain circumstances or stressors can cause a particular alter to emerge. The various identities may deny knowledge of one another, be critical of one another, or appear to be in open conflict. (2)
What is dissociation?
Dissociating is the experience of detaching from reality. Dissociation encompasses the feeling of daydreaming or being intensely focused, as well as the distressing experience of being disconnected from reality. In this state, consciousness, identity, memory, and perception are no longer naturally integrated. Dissociation often occurs as a result of stress or trauma, and it may be indicative of a dissociative disorder or other mental health condition. (18) Dissociative identity disorder is one of three dissociative disorders. The other two are, Dissociative amnesia is when someone cannot remember important details about themselbves or certain moments (usually extremely stressful or traumatic), more intensely than normal forgetting, And depersonalization or derealization disorder, when a person has an altered state of consciousness leading to feelings of dissociation or detactchement to ones surroundings or ones self, usually triggered by intense stress or experiencing/witnessing a disturbing event.
What is possession DID?
Possession-form identities in dissociative identity disorder typically manifest as behaviors that appear as if a “spirit,” supernatural being, or outside person has taken control, such that the individual begins speaking or acting in a distinctly different manner. For example, an individual’s behavior may give the appearance that her identity has been replaced by the “ghost” of a girl who committed suicide in the same community years before, speaking and acting as though she were still alive. Or an individual may be “taken over” by a demon or deity, resulting in profound impairment, and demanding that the individual or a relative be punished for a past act, followed by more subtle periods of identity alteration. However, the majority of possession states around the world are normal, usually part of spiritual practice, and do not meet criteria for dissociative identity disor-der. The identities that arise during possession-form dissociative identity disorder present recurrently, are unwanted and involuntary, cause clinically significant distress or impairment (Criterion C), and are not a normal part of a broadly accepted cultural or religious practice (Criterion D). (10)
What is non-possession DID
Diagnostic criteria (all = 6)
Disruption of identity characterized by two or more distinct personality states, which may be described in some cultures as an experience of possession. The disruption in identity involves marked discontinuity in sense of self and sense of agency, accompanied by related alterations in affect, behavior, consciousness, memory, perception, cognition, and/or sensory-motor functioning. These signs and symptoms may be observed by others or reported by the individual. 2 or more disticnt personality states (which may feel like possession), a loss in sensee of self or self agency, memory gaps in everyday life, gorgetting personal information, and trouble recalling traumatic events that differ from normal (notye that many of these symptoms are shared with other dissociatiuve disorders). (10) Recurrent gaps in the recall of everyday events, important personal information, and/ or traumatic events that are inconsistent with ordinary forgetting. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. The disturbance is not a normal part of a broadly accepted cultural or religious practice. Note: In children, the symptoms are not better explained by imaginary playmates or other fantasy play. The symptoms are not attributable to the physiological effects of a substance (e.g., blackouts or chaotic behavior during alcohol intoxication) or another medical condition (e.g., complex partial seizures).
How does DID develop?
Adolescence
Dissociative identity disorder is associated with overwhelming experiences, traumatic events, and/or abuse occurring in childhood. The full disorder may first manifest at almost any age (from earliest childhood to late life). Dissociation in children may generate problems with memory, concentration, attachment, and traumatic play. Nevertheless, children usually do not present with identity changes; instead they present primarily with overlap and interference among mental states (Criterion A phenomena), with symptoms related to discontinuities of experience. Sudden changes in identity during adolescence may appear to be just adolescent turmoil or the early stages of another mental disorder. Older individuals may present to treatment with what appear to be late-life mood disorders, obsessive-compulsive disorder, paranoia, psychotic mood disorders, or even cognitive disorders due to dissociative amnesia. In some cases, disruptive affects and memories may increasingly intrude into awareness with advancing age. (13)
Toggers to start DID
Psychological decompensation and overt changes in identity may be triggered by 1) removal from the traumatizing situation (e.g., through leaving home); 2) the individual’s children reaching the same age at which the individual was originally abused or traumatized; 3) later traumatic experiences, even seemingly inconsequential ones, like a minor motor vehicle accident; or 4) the death of, or the onset of a fatal illness in, their abuser(s).
What causes DID to develop?
- Did happens when a child with a nonfully developed personality faced prolonged and extreme abuse
- It is unknown why exactly people have DID, but a common factor among those with it is severe sexual and physical abuse during childhood
- Individuals with DID may have post-traumatic symptoms (nightmares, flashbacks, or startle responses) or post-traumatic stress disorder. Several studies suggest that DID is more common among close biological relatives of persons who also have the disorder than in the general population (3)
- Common factors; Individuals with dissociative identity disorder typically present with comorbid depression, anxiety, substance abuse, self-injury, non-epileptic seizures, or another common symptom. They often conceal, or are not fully aware of, disruptions in consciousness, amnesia, or other dissociative symptoms. Many individuals with dissociative identity disorder report dissociative flashbacks during which they undergo a sensory reliving of a previous event as though it were occurring in the present, often with a change of identity, a partial or complete loss of contact with or disorientation to current reality during the flashback, and a subsequent amnesia for the content of the flashback. Individuals with the disorder typically report multiple types of interpersonal maltreatment during childhood and adulthood. Nonmaltreatment forms of overwhelming early life events, such as multiple long, painful, early-life medical procedures, also may be reported. Self-mutilation and suicidal behavior are frequent. On standardized measures, these individuals report higher levels of hypnotizability and dissociativity compared with other clinical groups and healthy control subjects. Some individuals experience transient psychotic phenomena or episodes. (11)
- Common factors: Environmental. Interpersonal physical and sexual abuse is associated with an increased risk of dissociative identity disorder. Prevalence of childhood abuse and neglect in the United States, Canada, and Europe among those with the disorder is about 90%. Other forms of traumatizing experiences, including childhood medical and surgical procedures, war, childhood prostitution, and terrorism, have been reported. Course modifiers. Ongoing abuse, later-life retraumatization, comorbidity with mental disorders, severe medical illness, and delay in appropriate treatment are associated with poorer prognosis. (14)
When can DID develop?
- Did can develop at any age, but people usually have it when they have severe childhood trauma
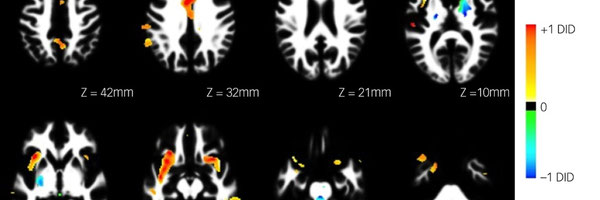
How does DID change the structure and anatomy of the brain?
Several brain regions have been implicated in the pathophysiology of dissociative identity disorder, including the orbitofrontal cortex, hippocampus, parahippocampal gyrus, and amygdala.
How does DID influence peoples lives?
- According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, more than 70 percent of people with DID have attempted suicide at least once, and self-injurious behavior is common among this group (4)
Memory
- The dissociative amnesia of individuals with dissociative identity disorder manifests in three primary ways: as 1) gaps in remote memory of personal life events (e.g., periods of childhood or adolescence; some important life events, such as the death of a grandparent, getting married, giving birth); 2) lapses in dependable memory (e.g., of what happened today, of well-learned skills such as how to do their job, use a computer, read, drive); and 3) discovery of evidence of their everyday actions and tasks that they do not recollect doing (e.g., finding unexplained objects in their shopping bags or among their possessions; finding perplexing writings or drawings that they must have created; discovering injuries; “coming to” in the midst of doing something). Dissociative fugues, wherein the person discovers dissociated travel, are common. Thus, individuals with dissociative identity disorder may report that they have suddenly found themselves at the beach, at work, in a nightclub, or somewhere at home (e.g., in the closet, on a bed or sofa, in the corner) with no memory of how they came to be there. Amnesia in individuals with dissociative identity disorder is not limited to stressful or traumatic events; these individuals often cannot recall everyday events as well. (9)
Function
- Impairment varies widely, from apparently minimal (e.g., in high-functioning professionals) to profound. Regardless of level of disability, individuals with dissociative identity disorder commonly minimize the impact of their dissociative and posttraumatic symptoms. The symptoms of higher-functioning individuals may impair their relational, marital, family, and parenting functions more than their occupational and professional life (although the latter also may be affected). With appropriate treatment, many impaired individuals show marked improvement in occupational and personal functioning. However, some remain highly impaired in most activities of living. These individuals may only respond to treatment very slowly, with gradual reduction in or improved tolerance of their dissociative and posttraumatic symptoms. Long-term supportive treatment may slowly increase these individuals’ ability to manage their symptoms and decrease use of more restrictive levels of care. (15)
Can DID be treated?
- The primary treatment for dissociative identity disorder is long-term psychotherapy with the goal of deconstructing the different personalities and integrating them into one. Other treatments include cognitive and creative therapies. Although there are no medications that specifically treat this disorder, antidepressants, anti-anxiety drugs, or tranquilizers may be prescribed to help control the psychological symptoms associated with it. With proper treatment, many people who are impaired by DID experience improvement in their ability to function in their work and personal lives. (5)
Identitiies (all from traumadissociation)
Identities often have separate skills, “roles”, memories, likes/dislikes, behaviour, assumed ages, genders, names and ethniciies, thought process, qand when that identity is in control the body can feel as though it has undergone physical change. FOrexample, if the identity i that f a small child, the body will feel as though it is psyicallly a small chuldr, even if its not. Alters often think they look different than how they actually look. psychobiological difference to others, e.g., different vision, medication responses, allergies, plasma glucose levels in diabetic patients, heart rate, blood pressure readings, galvanic skin response, muscle tension, laterality, immune function, EEG readings. (21) Different alters have shown different results in neuroimaging tests, including functional magnetic resonance imaging activation, and brain activation and regional blood flow and differences in PET scans. The variability between alters is measurably greater than variability between non-dissociative people who are attempting to simulate alters. [6]:121 Because many alters have a very different perception of their body, they may disown it, or believe strongly that it is a different chronological age, and refer to as "the body" rather than "my body".[6]:120,140 Alters who believe that they have their own, separate physical body, can result in refusing to seek medical care, and self-harm or suicide attempts, in the belief that they will be unaffected since it is not "their" body which is harmed. This can even involve attempting to kill off "others". One might need to negotiate with the alterz to tell them that by killing the body theyy also kill themsleves. (21)
Types of alters (19)
- each alyter is either a ANP\, assumed normal parts\, who is the host\, and EP\, emotional parts\, who hold the traumictic memories and can often get caught u or stuck in them. Host (the person who owns the body, handles everyday life and usually has no traumatic memories) Child alter, Often nicknamed "littles" or "little ones" are a common type of alter. Several child alters exist in most people with DID. Child alters often talk in a child-like way, but unlike a biological child they can normally understand abstract concepts and long words. They are often found to hold memories of child abuse which occurred at around the age the child alter feels he/she is. [7]:18 Some may have the speech or appearance of a very young child, the youngest being unable to talk, read or write. [7]:18 Child alters may gradually age of may remain the same age. Some child parts may hold feelings of terror and pain, while others may be playful and fun-living and have only positive memories. [16]:60 A child alter may also be an idealized representation of the "perfect child" from the "perfect" family, for example the "good boy". [7]:18 Child alters should not be confused with the concept of having an "inner child", which applies to non-dissociative people., Core, Core personality or core self is a term rarely used now in scientific information. Instead, all people including people with DID are believed to be born with multiple original discrete "behavioral states", which fuse into a single core personality by around age 5/6 during a relatively normal early childhood, but in DID this process is disrupted and the behavior states either remain separate and begin to become increasingly independent, or they split off futher alters. [6] Despite this, some people with DID do identify as having a core self/original personality, and people with DID are not required to perfectly fit current theory in order to meet the diagnostic criteria. For example Chris Costner Sizemore, whose MPD was described by the 1950s movie The Three Faces of Eve, experienced "Eve White" as being her original personality.[7]:11 (Years later, Sizemore discovered an additional 21 alters/parts, which she described in her books). The DSM-III description of Multiple Personality included the term "original personality", described as usually the "subpersonality" whose name was the same as the person's legal name, "original persoonality" which was removed in the, Dead alters, Usually this is an alter hidden from the rest of the system, often in a memory of a trauma in which they felt they were being killed. The child who survives a near-death experience may develop a "dead alter" to contain this experience.[16]:64 Alters can"t really die or be killed since the person"s brain is still alive, their feelings will still leak through into other alters. "Dead" alters can be revived. Introject, Like alters based on fictional characters or people known to the person with DID, these alters are internalized representations (introjects). They are rarely described by psychotherapists and psychiatrists, except when referring to survivors of ritual abuse. Examples in military/political abusive groups include child alters who believe they are Hitler, famous doctors, generals, or other military leaders. [9]:337 There may be several alters who each believe they are the actual person they are based on, and are unaware of one another - e.g., several "Hitler" alters in the same person. [9]:337 In ritual abuse with 'religious' beliefs, alters may believe they are Jesus, or supernatural beings like God or Satan. [9]:325, 327. Unsurprisingly, a person who has an alter claiming they are a famous person may be misdiagnosed as having Schizophrenia or a Psychotic Disorder, because claiming to be a famous person is common is psychotic disorders with delusions. Psychotherapist Alison Miller gives the highly unusual example of a person who developed alters that were copies of Axl Rose and rest of Guns'N'Roses band - and was misdiagnosed with Schizophrenia as a result. [10]:2 In DID/DDNOS, however, an alter can adapt their beliefs if presented with clear evidence that they are not that person, for example that Hitler is dead and the Nazis lost the war, because logical thinking remains.[9]:101 Note: Delusions can also exist in people with DID/DDNOS if they have a Psychotic Disorder or Schizophrenia as well. Opposite sex alters, Presectutor, Protector, Teen alter, suicidal alter, and sexual alter are all common in people with DID. Some of the less common include, Demon alters, Demon and demonic alters are a type of spirit and supernatural alter but are not actually supernatural beings and may result from spiritual abuse and an abuser who blames the child for the abuse.[6]:170 In abusive groups, a young child can be severely traumatized in order for abusers to intentionally create an alter, and the alter can be tricked into believing they have been possessed by, and have become, a demon. Some survivors report being dressed to look like a "demon" with costumes and theatrical makeup, and being told to look in the mirror and told that they are a demon. Hallucinogenic drugs may also be used to cause supposedly "spiritual" experiences. [9]:68,337 Some demon alters may be told they are animals. They may be very intimidating, with names such as Demon, Lucifer, Satan or Devil, however they should be able to engage with psychotherapy, and all alters should be accepted.[16]:61 These "demonic" or "evil" alters may have the role of maintaining loyalty to the abusive cult which created them, in order to keep the whole person alive. They are often a form of protector known as a persecutor.[11]:142 [9]:337-338 These alters are usually hurt children who have been tricked into believing they are "evil", and may have been tricked or forced into harming others. With "patience, persistence and kindness" they can be allowed to choose a different role once the person is safe from abusers. Attempts to banish them using religious techniques such as "deliverance" or exorcism do not work permanently, can be harmful and may prolong any internal war between alters and preventing healinhg, Disabled alter, Alters may be disabled when the person's body is not, for example a blind or mute alter may be created in response to an abuser's instructions, e.g. "Don't talk", "You didn't see anything", resulting in involuntary psychosomatic symptoms which come and go, rather than a permanent physical injury. These disabled alters can regain their sight, hearing, or mobility, etc. during healing, for example, after working through the memories that caused their disabilities or when switching to a different alter personality. [9]:34-35 This psychomatic expression of the impact of trauma typically results from somatoform dissociation, which is when psychological trauma or conflict is expressed as physical rather than psychological symptoms; the Somatic Dissociation Questionnaire 20 (SDQ-20) is a screening tool for DID that assess physical symptoms only.[6] Severe physical symptoms may result in the additional diagnosis of Functional Neurological Symptom Disorder (DSM-5), formerly known as Conversion Disorder, which can also occur without DID. Psychogenic or non-epileptic seizures are particularly common physical symptoms in people with DID, but can occur in other people.[6] Caregiver alters, Caretaking alters are a type of a protector, they help manage and care for other alters, and sometimes external people (for example children). [24]:83 They are often motherly, and may be modeled on a real person. [16]:61-62 Caretaking alters lack awareness of self-care and become exhausted easy; they only have a limited role and have little capacity for play, exploration or socializing. Robot alter, Supernatural being alyter, Animal alter, Abused children may develop animal parts/alters because they identify with animals and consider them friends. Animal parts may be able to express emotions that the Apparently Normal Parts can"t. Animals like tigers may function as protectors, growling when an Apparently Normal Part is distressed. [16]:65 Alters may also become to believe they are animals because abusers either told them they were or treated them like animals, e.g., dog alters. Some abusers are known to force children to act like animals, for example making them bark or use a dog bowl for food.[18] Animal alters may also be created if the person was forced to harm others, as a way of containing the guilt of having to act in a way which feels more violent and animal than human. Complex trauma can leave even a non-dissociative person feeling "inhuman".[16]:65, [23] Animal or animal-like alters should be accepted, and treated just like any other alter.[9]:69, [6]:133,[6]:139 Animal alters can be taught that they are actually part of a human body, and can adapt. For example, a snake alter may be created when a child has arms and legs bound, and be tricked into believing that, like a snake, they do not have arms or legs.[9]:69 Animal alters often have a definite gender and can present, and be accepted, as human, without the person necessarily being aware they are communicating with an animal alter or any alter at all.[18]:55 Read more: https://traumadissociation.com/alters Political/military alter, And Subparts, And the non humans ones dont know that they aere infact human. Fictives/Fictional characters Alters may be created which are internalized representations (introjects) of fictional characters. Some people with DID refer to alters based on fictional characters as fictives although this term was not used in literature on DID until 2021, before then fictives were described in many case studies and books, but had not been given a collective term.[9],[32],[35],[43] People with Maladaptive Daydreaming (MD) often have groups of inner characters based on fictional sources, but these are different to alters in DID because they cannot physically take control or interact with other, outside people, and are not split-off parts of the person's own personality, although there are other differences as well. Like any other alter, alters who are fictives can physically take control of the person's body.[1] The characters that alter personalities are based on may come from sources like nursery rhymes, fairy tales, children's stories or books, music, games, movies and other sources.[36]:493, [43] One good description of therapy with several alters based on fictional characters comes from a case of DID in Turkey published in 1997: a woman aged 45 with a severe abuse history was found to have Dissociative Identity Disorder, and two of her alters were based on the classic story Snow White. "Two identities had been formed from childhood imaginary playmates: "Pamuk Prenses" (Snow White) and "Kraliçe" (The Queen). They both enjoyed parties at nights where the Queen looked after, protected and controlled the young "Pamuk Prenses" and enviously competed with her at the same time. Snow White danced and sang. When Snow White took control she saw her husband and children as "the relatives of that poor woman in the neighborhood" (Sad Halimé [another alter])... These identities had been formed at about the age of twelve; they knew the other personalities, but they saw themselves as distinct from all the others. — Tutkun & Sar (1997) [32]:151 Some abusive groups/cults have been known to traumatize children in order to force them to create alters based on particular characters which suits the needs of the abusers. Ritual abuse survivors in particular report being forced to create alters based on many different fictional characters, including: characters from Lewis Carroll's story Alice in Wonderland, which has been made into several movies [39] An “everyday life” alter based on the character “Samantha” from an episode of the TV show "Bewitched" [36]:523 Charles Wallace and Meg (from Madeleine L'Engle's 1962 book A Wrinkle in Time) - as part of MK-Ultra ritual abuse[37]:70:72 Peter Munk (a character from a German fairytale) who is "unemotional, obedient, lacking in self-awareness" and motivated to avoid pain, reported in a German survivor of ritual abuse during the "cold war" [35]:80 Sleeping Beauty, who believed she was dreaming when actually working as a government agent (as part of MK-Ultra) [37]:217,272 Tinker-Belle (from Peter Pan), in a survivor of Monarch programming/ritual abuse [38]:108-109 The Wizard of Oz, including the scarecrow (who was told he had "no brain", he was obedient and suggestible), the cowardly lion (who held the emotion of fear), tin man (who was told he had no heart - meaning no empathy, and as such was able to be a trained killer following someone else's orders)[39]:62 All alters may adapt and change over time, and some may even choose to take on the form of fictional characters if that serves a helpful purpose. Dr Colin Ross,
a well known psychiatrist and Dissociative Disorders specialist, states that a group of demonic alter personalities in a survivor of Satanic Ritual Abuse chose to transform their identities to become Ewoks (from Star Wars) as part of healing.[33]:153 Fragment, Some alters are very limited in their role, for example they may only have a small number of emotions, hold particular isolated memories or have a very limited job. These 'partial' alters are sometimes known as fragments. [10]:280 Fragments can either have a range of emotions but only a limited life history, or a more substantial life history but be unable to feel a range of emotions (for example, always sad, either angry or fearful). Special purpose fragments are even more limited, for example existing to carry out a very limited role and never acting beyond that. Memory fragments hold a very limited knowledge of an event, and only experiencing very limited emotions. [4]:xii:xiii Several fragments together may hold a single event. [11]:6, 143 Gatekeeper alter This type of alter has the job of keeping traumatized alters from appearing. [16]:58 They may also hold back memories or control which alters can take control of the body, and when. [9]:54 Host, Presenting Part, Front Person, or Fronter The personality part/alter that "has executive control of the body for the greatest percentage of time during a given time period."[4]:xiii A person with DID will have more than one host over their lifetime. [16]:59 See Apparently Normal Part of the Personality. Insiders This term covers many different kinds of alter who are not primarily responsible for everyday life, they often hold trauma memories. They often have been so separated from everyday life that they are unaware of the years that have passed and often do not know that the body has physically grown up. [9]:30 See Emotional Part of the Personality. Internal Self-helper (ISH) These alters are helper parts. They have extensive understanding of different alters and how they work together, and often help by explaining things to the therapist. [16]:64 Also known as Managers or sometimes Inner Self-Helpers. Introject / Copy Alter These alters believe may they are another person entirely, such as an abuser or a close relative. [9]:34 They have the characteristics of another person, for example a paternal introject with the behaviors and views of a person's abusive father. [7]:18 Introjects which are mimicking abusers are trying to "keep you inline" in order to protect you from external abusers.[9]:33 "Introject" is a term used in general psychology to refer to taking on and internalizing the views and thoughts of others without reviewing them.[17]:259 This is part of normal development in early childhood, these introjected parts/aspects of a person can be either healthy and helpful, or abusive. For example, an adult verbally abused as a child may have an introject which states "nobody likes you" or "it's a dog eat dog world" - both of these would negatively affects a person's likelihood of making friends. In people without DID/DDNOS, introjects will not be alters, but become incorporated (introjected) into their personality. Introjects can change with psychotherapy. Also see maladaptive daydreaming (inner characters created by daydreaming, which are not alters). Military and Political Alters Alters may be soldiers of different ranks, or believe they are well known political leaders. These alters are often been created within abusive groups with a particular set of political/military or religious beliefs, the alters are indoctrinated to force them to take on the beliefs of the group.[9]:61-63 They may have titles of military ranks, like generals, or names like Hitler. Groups which are known to have carried out ritual abuse using dissociation to create alters include the US government (e.g., MKUltra, which included many Nazi doctors operating on behalf of the CIA), neo-Nazi groups, and white supremacists including the Ku Klux Klan. [9]:18, 54 See demon, demonic and 'evil' alters, for alters which are copies of actual people see introject. Opposite-sex alters and different gender identites in alters Some alters may have a different gender identity, and/or genuinely believe that their body has physically different sexual organs than it actually does, for example a male alter in a physically female body, who may or may not be aware of having no penis (a severe level of dissociation is present in DID, which may include amnesia for puberty, somatoform dissociation causing a lack of bodily sensations, "out of body" experiences, and/or severe subsconscious avoidance of the body). Opposite sex alters are usually more like a young girl's idea of how a boy would be an actual boy, or a young boy's idea of how a girl would be, based strongly on cultural norms or stereotypes. Normally they have personality traits which associated with the gender of the opposite sex. A female alter in a male body may be very fearful or frightened, and a male alter in a female body may be very angry, feel physically strong, or be very brave. An alter may be have an opposite gender because of sexual abuse, for example a male alter does not have vagina, so will not fear being vaginally raped as the female body was. A female alter may be created in a male because that alter was forced to take on a female role in having sex with men, although opposite-sex or differently-gendered alters do not automatically mean that child sexual abuse was the cause. Trance logic is characteristic in DID, and involves beliefs that are not delusional but also not in keeping with physical reality, as described above; another example would be for an alter to believe that they do not live in the same body as the patient or the other alters, and may be invested in killing off others, wrongly believing that they can live on without a body. [9]:34-35 Nonhuman Alters Alters are the result of severe dissociation; they are "constructed by the 'logic' of dream or trance",[30]:184, and can be strongly influenced by a person's culture.[1]:294 As a result, alters can take any form; some alters may not view themselves as human, and may either feel (or fully believe) that they are not part of a human being. They may view themselves as having a different physical form (or no physical form at all, for example a spiritual being [6]), this is recognized within the DSM-5's description of DID. [1]:294 Prolonged and severe interpersonal trauma can leave a person feeling "no longer human", and has been reported in people with Complex PTSD and OSDD, for example as a result of being a prisoner in a concentration camp, being a political prisoner in a country with a poor human rights records, or as a result of severe child abuse. [16]:65, [23] Given the trauma history of the vast majority of people with Dissociative Identity Disorder and OSDD, it is unsurprising that parts of the mind may have taken on a nonhuman identity. Some examples include alters that identify as animals, demonic or 'evil' alters, spirits, ghosts or spiritual beings,, mythical figures,[1]:294,[30]:184 robots or machines, or even inanimate objects [9]:47. Some people with DID or DDNOS refer to such alters collectively as "otherkin", although the word otherkin can have different meanings, including meanings not relevant to Dissociative Disorders. Object Alter Alters which identify as inanimate objects are a type of nonhuman alter, for example a tree.[24]:80 Alters can also be hidden inside animate objects, for example inside natural-looking structures in the inner world, e.g., mountains, trees, lakes or rivers. [9]:49 Persecutor A common type of alter, often acts in a harmful way but there is a protective logic behind a persecutor's actions. [7]:17-19 Persecutors often have a distorted view of reality\, and may disrupt therapy or intentionally injure the person's body\, for example to punish child alters for disclosing abuse that has been kept secret. All alters "should be treated with equal kindness\," despite their behaviors\, and persecutors are often seen as "misguided protectors" which can be negotiated with.[9]:41\, [28] Some persecutors may threaten to "kill off" the ANP (host) and appear to have no positive or protective intentions\, however these can still be engaged with.[29]:95 Some persecutors may be introjects of abusers. Download Therapeutic alliance with abuser alters in DID for more information on responding to a persecutor. Protector Protector alters are common\, there are three main types: 'fight' parts\, persecutors and caretakers. The 'fight' parts and persecutors are types of EP which have defensive intentions\, despite their often self-destructive behaviors such as self-injury or eating disorder behaviors.[24]:82-83 The term 'fight' does not necessarily refer to violence\, but to the 'fight' reaction present in PTSD\, which often involves verbal aggression.[1]:143 A diagnosis of DDNOS or Dissociative Identity Disorder is not associated with crime or "wild aggression".[26] [27] Therapist Jo Ringrose\, who has considerable experience of working with alter identities\, states that violent alters exist\, but has never met one. [27]:8 Protector alters try to manage rage and anger\, and avoid feelings of hurt\, fear or shame. They focus on perceived threats\, and find dependence\, emotional needs and close relationships (attachment) threatening. Protectors may view themselves as a very tough child or teenager\, a powerful animal\, or a physically strong\, adult male. They can act internally\, or show external hostility\, e.g.\, telling a therapist that other alters don't need them and warning the therapist to leave them all alone. Defensive "acting out" may be directed at a therapist or others close to the person; the ANP may have no behavioral control or memory of it. However\, the "whole person" (all alters collectively) should still be held responsible for the behavior of all parts.[6]:132 A protector may follow an alter that is "needy and searching desperately for attachment" in order to protect it.[24]:87 Internal perceived threats may include the crying and dependency needs of a traumatized child part\, which an internal persecutor may silence with rage or self-harm. [24]:82-83 Protector parts may see the partner of an ANP (host) as a threat\, for example the partner initiating sex may cause a switch to a protector alter\, who perceives it as an attempt to rape\, and fights off the partner. [24]:74 Communication and negotiation can improve safety\, and no attempts should be made to "get rid" of any alters.[6]:132-133\, [6]:139 “With DID patients\, if they feel hostility or aggression they take it out on themselves with self-harm... They’re self-destructive and repeatedly suicidal\, more so than any other psychological disorder. So that's what's typical – not this wild aggression\, or stalking women..." — Dr Bethany Brand [25] Psychotic Alter Some alters have psychosis or psychotic symptoms. However, many symptoms which appear psychotic are not. For example, visual flashbacks may be mistaken for hallucinations, and strange body sensations (body memories) which are physical flashbacks of past trauma can be mistaken for tactile hallucinations. [12]:64 Hearing "voices" is a common experience in people with DID/DDNOS, the "voices" are alters trying to talk, and occasionally may come from outside the person's head rather than inside, which is more common. "Thought snatching" (taking away your thoughts) can be caused by the actions of alters. Beliefs caused by trauma can be mistaken for paranoia, for example a person may be told that a "bug" has been implanted by abusers to record any dislosures they make. Working through the memory of the trauma will resolve the paranoia that it caused. [9]:129 Some people who have been abused within ritually abusive groups may have alters who are trained (programmed) to produce psychotic-like symptoms under certain circumstances.[9]:142 It is possible to have an alter with a psychotic disorder\, or to have schizophrenia as well as DID/DDNOS. [1]:291-307 This appears to be relatively rare. Schizophrenia is a common misdiagnosis for people with Dissociative Identity Disorder\, although many people with DID/DDNOS believe they are going "crazy" they do not have a break with reality.[7]:58-59 Abusive groups are known to have created alters who carry out "jobs" which make a person appear either "crazy" or learning disabled\, for example scrambling or garbling words and numbers so they cannot be understood\, hearing high pitched sounds and feeling "lost in a maze" in the back of your head\, making your mind go foggy or misty or being spatially confused and unsure what the truth is.[9]:78\, 80-81 Anti-psychotic medication will not "remove" alters but can make the communication needed to heal more difficult.[9]:129 Robot or Machine Alter Alters who believe they are robots or machines, and have no understanding of emotions, have been reported in survivors of ritual abuse. These alters were told they were robots or machines, and were not allowed to feel any emotions, were trained to follow instructions and not to think, and may have been made to believe that they cannot move.[9]:68 If a large number of similar robot parts exist, it is more effective for them to agree to fuse (integrate together permanently) rather than repeating the same therapy with each. Robot and machine parts are actually part of a person, and can be helped to feel more human, and to learn how to think for themselves, rather than just responding to the instructions past abusers gave. [9]:142-143 Sexual Alter Sexual alters may be created to handle sexual abuse and rape, and to keep that knowledge away from other parts. One alter or group of alters may handle sexual abuse from men or boys, while others are created to handle sexual abuse and rapes from women or girls. [22]:77 Shell A shell alter is an Apparently Normal Part (host alter/front person) which handles daily life and is designed to hide the existence of other alters from the outside world. [10]:33 Shell alters do not exist in DID, they only exist in one form of DDNOS (now renamed to Other Specified Dissociative Disorder). The apparently normal part (ANP) is a shell through whom the inside parts/alters act. The inside parts can come near the surface, temporarily blending with the ANP. The inner parts are not regarded as separate, distinct states although amnesia may exist between them. [7]:9, [9]:5 If DDNOS is caused by ritual abuse and mind control, the shell alter is not supposed to know about the others.[9]:5 Spirit, Ghosts, Supernatural beings and 'Possession" Alters These types of alters are referred to directly in the DSM-5 diagnostic manual, underneath the diagnostic criteria for Dissociative Identity Disorder. Some people have alters which are all spirits, ghosts or supernatural beings such as angels or genies. These are regarded as possession-form identities, if a person is consciously aware of the actions of the alter then the person may describe themselves as feeling "possessed" by an outside person, spirit, deity (god), demon, or a "ghost", for example of a person known to them who has died. [1]:292 Possession-form alters are not part of normal cultural possession experiences, they are involuntary, recurrent and distressing. [1]:294 Animal alters are also common in this form of dissociation.[1]:293 People can also have one or more of this type of alter along with other types, for example child alters or protectors. Alters who believe they are spiritual or supernatural beings should be treated in the same way as any other type of alter identity, with psychotherapy (talking therapy). Exorcisms are known to be harmful and ineffective in treating complex dissociative disorders, and attempts should not be made to "get rid" of alters. Instead they should be understood as a way of coping with traumatic life experiences. [6]:170-171 Sub-parts An alter may have another dissociated part inside, which has a different role or function. [9]:141 Subsystem A subsystem is not a type of alter but the name for a group of very closely related alters which may have formed by splitting off all at the same time, either splitting off from an existing alter undergoing massive new trauma (effectively this means an alter has their own group of alters), or from the ANP/host being extremely traumatized by a new trauma. A subsystem can also form by alters splitting off from an existing alter at different times, which is not necessarily due to major trauma but is still psychologically essential for survival. When a new trauma is not bearable for either the existing alter or a new alter, the feelings and/or memories are split across several new alters instead, these alters may be extremely limited fragments, for example holding only part of a memory.[9],[10],[11] People who are polyfragmented typically have multiple subsystems, but having subsystems is not an indicator of being polyfragmented.[6],[9],[10],[11] Suicidal Alter/Internal Homicide A common type of alter.[24]:79 If somone with Dissociative Identity Disorder or DDNOS is suddenly suicidal, this may be due to the influence of a suicidal alter, although the ANP (host) themselves may be feeling suicidal.[24]:75, 306 According to the DSM-5 psychiatric manual, over 70% of out-patients with DID attempt suicide and multiple attempts are common. Amnesia can make it difficult to assess the suicide risk, and there may be amnesia for a suicide attempt. [1]:295 Some alters may be unaware that they share the same body as the ANP, and believe that killing off the ANP or others will not harm them; this increases the suicide risk further.[6]:132, 140 See persecutor for alters who are threatening to kill the ANP (host). See Negotiating with alters Teen alters Teenaged or adolescent alters may occur in people who had significant trauma during those years, or they may be child alters who have grown older.[7]:18 Twin alters Twin alters are two alters of the same age who are normally opposites of each other in views and behaviors. Twin child alters are common, for example one may love the abuser, be eager to please and have only positive views towards him/her, and another may hold angry and rejecting views towards the abuser. [16]:61 Suicidal or homicidal alters are very common. Not all alters who are suicidal/homicidal fall under this category, but these alters are often unawaree that they share a body with the other alters, or be under the belief that killing themselves will only harm them, not all the other alters. Over 70% of people wit DID have attamtped suicide, though not all of thge have these alters. The alters a person has depend on what that person needs to survive, for example, there is a protector to protect them from the abuse, and an internal self jelper to internally help the person.
Amount of alters
The amount of offers differ, and a1984 study found that peoolle had two to over 100 different alters, and 50% had 1) or less, and 50% had 11 or more. Women tend to have more, with an average of 15 alters per woman, ewhereas 8 per man. Some have polyfragmented parts, meaning their alters are very close in identity, so theyre identity count ranges in the hundreds People usually find the existence of more altrs during treatment, with the average person having 2-4 known alters at diagnosis, and find another 13-15 during treament. Ths is because the treatment will make the alters feel more aaccepted or free to express their being or their triggers, so theeyy feel more pree to communication and to come out of hiding. (18)
Polyfragme nted DID
Most say that poly frwgmented DID must have 100+ alters, but others say “dozens”. They arw so many because the aters are spilt into fragments. Many use the same name or even no name. This all results in less obvious swicthing between alike alters. Trauma which is severe or/and long lasting and organized, like cults, ritual abuse, pedophile rings, human trafficing, or other sadistic extreme abuse over a long period of time with multiple abusers. Since they are all so close in identity and prose they can sometimes fuse together, or the alike obes can, 10 at a time
How do they interact?
Individuals with dissociative identity disorder may report the feeling that they have suddenly become depersonalized observers of their “own” speech and actions, which they may feel powerless to stop (sense of self). Such individuals may also report perceptions of voices (e.g., a child’s voice; crying; the voice of a spiritual being). In some cases, voices are experienced as multiple, perplexing, independent thought streams over which the individual experiences no control. Strong emotions, impulses, and even speech or other actions may suddenly emerge, without a sense of personal ownership or control (sense of agency). These emotions and impulses are frequently reported as ego-dystonic and puzzling. Attitudes, outlooks, and personal preferences (e.g., about food, activities, dress) may suddenly shift and then shift back. Individuals may report that their bodies feel different (e.g., like a small child, like the opposite gender, huge and muscular). Alterations in sense of self and loss of personal agency may be accompanied by a feeling that these attitudes, emotions, and behaviors—even one’s body—are “not mine” and/or are “not under my control.” Although most Criterion A symptoms are subjective, many of these sudden discontinuities in speech, affect, and behavior can be witnessed by family, friends, or the clinician. Non-epileptic seizures and other conversion symptoms are prominent in some presentations of dissociative identity disorder, especially in some non-Western settings. (8)
How are they created
- To deal with intense trauma or daily changes that the person cannot deal woth alone
- Somempeople can recall spefici wevenets or things that caused the creation of different alters ea a Native American man described having animal and spirit alters which were created by a mixture of starvation, severe beatings and hallucinogenic herbs or drugs. His wolf alter was created after beatings for failing to communicate with the "wolf spirit", the wolf alter took on the characteristics he attitrubed to wolves: widsom, cunning and wolf-like behaviors. The wolf alter both allowed for the trauma to be handled and was able to use its characteristics to diagnose illness and manage complex life situations. (19)
Switching
Each did system is different Switching involuntarily canbe embarrassing, frustatioating, or shameful to people with did, but with communication with their system theu can come up with a list of terms and conditions fir when they come out Switching might be consenual, forced, or triggered Switching is process of going from one alter to another. This process looks different for every system, but for many it’s embarrassing, frustrating, and definitely one of the biggest ways DID effects peoples social interactions and function. Through the right treatment, alter can make rules around who has control when. Signs of switching include; hearing internal voices of other alters, an inability to think clearly, feeling psycically changes in the body from another alters emotions, a feeling of being “mioved out of the way”, feeling detached, stress from not knowing what has or will happen and an overall detachment from ones body. Tiggers to switch include; overstimulation fo any sense, uncomfortable emotions, certain times or the year, good/bad memories, extreme anxiety, or someone saying an alters name.
Signs of switching
- Hearing a headmate's voice in my head
- My head goes foggy
- I cannot concentrate, process information, or think clearly
- I hear outside voices from afar, as if in a tunnel
- My head feels chaotic
- I can physically feel my facial affect changing and my emotions flooding my facial expression
- My handwriting changes, sometimes from messy and precise or from print to cursive
- I stare blankly at the wall or floors and "feel" myself being moved out of the way
- My eyes change shape and color
- Shivers run through me as though I'm cold
- I feel detached from myself as if someone else is "running the show"
- I have headaches that cannot be relieved with medication
- I feel dizzy and light-headed
- My thoughts get louder
- I do not make eye contact
- I take a deep breath and breath an enormous sigh as if to alleviate building stress
- I look around the room suspiciously as if I'm unaware of my surroundings
- I frequently watch the clocks to account for time lost (25)
Triggers to switch
- good/bad memories
- Any of the five senses
- Strog, uncomfy feelings
- Eztreme stress
- Certain times of the year
- Looking at old pucs
- An outsider saying alters name
- Extreme anxiety
- Noises
- Crowed soaces
Why does a person switch?
- The overtness or covertness of these personality states, however, varies as a function of psychological motivation, current level of stress, culture, internal conflicts and dynamics, and emotional resilience. Sustained periods of identity disruption may occur when psychosocial pressures are severe and/or prolonged. In many possession-form cases of dissociative identity disorder, and in a small proportion of non-possession-form cases, manifestations of alternate identities are highly overt. Most individuals with non-possession-form dissociative identity disorder do not overtly display their discontinuity of identity for long periods of time; only a small minority present to clinical attention with observable alternation of (7)
- During childhood the alters can often act as a protector, comforter or parental igure to the main person, so during abuse they may swicth to another personallity
How many people have it?
- In the usa, 1.5% people have it, about 1.4% of females, and 1.6% of males
How does DID affect different people?
Gender differences
Females with dissociative identity disorder predominate in adult clinical settings but not in child clinical settings. Adult males with dissociative identity disorder may deny their symptoms and trauma histories, and this can lead to elevated rates of false negative diagnosis. Females with dissociative identity disorder present more frequently with acute dissociative states (e.g., flashbacks, amnesia, fugue, functional neurological [conversion] symptoms, hallucinations, self-mutilation). Males commonly exhibit more criminal or violent behavior than females; among males, common triggers of acute dissociative states include combat, prison conditions, and physical or sexual assaults. (16)
Cultrual Differneces
Many features of dissociative identity disorder can be influenced by the individual’s cultural background. Individuals with this disorder may present with prominent medically unexplained neurological symptoms, such as non-epileptic seizures, paralyses, or sensory loss, in cultural settings where such symptoms are common. Similarly, in settings where normative possession is common (e.g., rural areas in the developing world, among certain religious groups in the United States and Europe), the fragmented identities may take the form of possessing spirits, deities, demons, animals, or mythical figures. Acculturation or prolonged intercultural contact may shape the characteristics of the other identities (e.g., identities in India may speak English exclusively and wear Western clothes). Possession form dissociative identity disorder can be distinguished from culturally accepted possession states in that the former is involuntary, distressing, uncontrollable, and often recurrent or persistent; involves conflict between the individual and his or her surrounding family, social, or work milieu; and is manifested at times and in places that violate the norms of the culture or religion. (17)
Ritual abuse DID
Definition
Although different definitions of ritual abuse exist, very few apply only to abuse with only "occult" or "Satanic" elements. Over time, the definition of ritual abuse has evolved; newer definitions include the same types of abuse but apply equally to secretive military/political or organized crime groups rather than only religiously based abuse or cults. [19]:9-10 An newer definition of ritual abuse states that:Ritual abuse is "Repeated, extreme, sadistic abuse, especially of children, within a group setting. The group's ideology is used to justify the abuse, and the abuse is used to teach the group's ideology. The activities are kept secret from society at large, as they violate norms and laws." (21) Ritual abuse victims experiences often share many similiarties to the treatment of politcial prisoners, such as,
- Extreme pysical and emotional torture,
- Distortion of lahnguage, truth, meaning, and reality
- Sham killings,
- repeated near death situtaions or being threatened by death,
- Being forced to hurt others,
- Being forced to watch the abuse of others,
- Being forced to make im[ossible choicezs,
- Having boundaries severely crossed, forced nakeedness, shame,, and embarrassment,
- Hoaxes, set up, tricks, and testing
Abusers
There are four main types of perpetrators of ritual abuse:
- multigenerational family groups, where generations of children are raised within the abusive group and may be trained to become perpetrators
- self-styled abusive groups
- lone operators such as serial killers, and
- "dabblers", who are generally the least extreme perpetrators of ritual abuse, may be adults or teens [21]:44
- in the case of children, day-care or preschool, and community-based groups of perpetrators also exist (22)
Organized abuse
Ritual abuse falls undeer organized abuse, which us extremely sadistic and extreme, along with, Network abuse, caused by people apart from family, Institualional abuse, child sexual abuse cayused by an insttitution, Familial organzied abuse, sexual abuse against a child in the family, and the abusers often let people outside the family hurt the child(ren)
Forms
RItual abuse is found in religous/spirit7ual groups, but also in military and politcial settings.
Satanic ritual abuse (religious ritual abuse example)
This is the first kund of rutual abuse known waas satanic ritual abuse, in which “Satanic Ritual Abuse is a form of ritual abuse that involves the use of a combination of Satanic elements such as symbols, objects, and beliefs during abusive rituals” (23)
PRoject MKUltra (political/military abuse)
MkUltra was a project done the USA intelligence aganices, like the Cia, that involved taking NAzi doctors and scientists who commited crimes, such as unethical experimentation against children and adults. One aim of MKUltra was to take the amnesia part of DID to make spies and assassins whoo were not consciously aware of their actions/ involvement.this also meant that if they were interrogated or tortured they wouldnt be able to say information they knew because they couldnt remember
Implications
- Those who experience ritual abuse often have PTSD(POST TRAUMATIC STRESS DISORDER) or DID later on in life
- DID only occurs if the abuse starts early on in life
- `Others who have experienced ritual abuse also experience addiction, bipolar dissorder, depression, anxiety, dissociative amesia, allof which are common in trauma survivors/ those with PTSD
Cases
Louis Auguste
Louis Auguste Vivet, who lived in France in the 19th century, was one of the first people described with Dissociative Identity Disorder, and also experienced paralysis. Vivet had long episodes of disabling leg paralysis and sometimes total paralysis which came and went; this was related to psychological trauma caused by a snakebite rather than physical injury. Before the snakebite, Vivet had already DID, which was highly likely to have been caused by early and prolonged childhood abuse, which included him developing a thief alter to survive after being abandoned and left homeless at age 8. [55] "Louis Auguste's case of DID was documented during the 1880s by his attending physicians. Louis was abused during childhood, became a thief when he was eight and sentenced to a rehabilitation centre. Louis was bitten by a viper at the age of 17 and experienced leg paralysis, then he was transferred to an asylum to study tailoring. At age 18, he was released from the asylum, went to visit his mother, and continued his agricultural work. Unfortunately, he was admitted back into an asylum as he suffered from a conflicting range of symptoms such as total paralysis to completely no symptoms. This hemiplegia was however noted as odd as the patient could walk while under hypnosis by the attending physician. During his hemiplegic and antagonistic state, Louis was noted to not have any recollection of his stay in the asylum when he was 17, but had total recollection when he reverted back to his calm state. There were also records of him inexplicably losing and finding objects he had no memory of, alternating personalities shown through complementary actions of thievery and of diligent agricultural work, and differing somatic symptoms.10,11 Louis manifested symptoms of DID which include a disruption of identity and episodic memory loss not caused by substance."12 — Surawijaya et al. (2023)
Margo
Disabled alters are more likely in people with related physical disabilities, for example the case of Margo, a woman with psychogenic blindness caused by DID also had physical eye problems, and had a child alter who could see
55 year old vcacausian woman
A woman with a history of substance abuse disorder and comorbiid bipolar disorder came to local general hospital with a history of a fragmentated personality that turnt tomultple, under the influence of drugs and emotional stress. Switches occured anytuime and were involuntary causing the assumed normal parts anxiety, but they wrre esoecially more vommon during stressful situations of substnace abuse More report violnece and harm dobe durung one on one visits vs group visits Her personaliuties were
- That of a seven year old girl,
- A personality that behaved as a teenager,
- A malle,
- Her ANP, the 55 year old woman who the body belonged tto,
She reported that stressful situations and substance abuse would trigger her multiple personalites During switching she wa violent to people, even those close to her. She was suicidal and homicdial, resulyting in two hpast arrests. She had to restrain and put herself into isolation by locking her self in a room, then calling the police. While under the influence if drugs like cocaine and mariguana, her eprsonaluty spilt into multiples ones, tat differed in age and gender.
Seven year old alter
- Had a moody and self arrogant personaluu=ity
- This alter would hurt herself or hace weeping spells if her wants werent met
Teenage alyter’
- Sharo choices and dressing
- Increases in substance abuse, alcohol use, and smaoking, leading to multiple causes of fights or homicidal attacks, and even instances of self harm
- Mant+y scars were found ib the dorsal side of her right hand
- Pressured and repetitive speech
Male alter
- Voice and behavour change
- Male dressing, language and prescription off male body parts, male choice of frends, female ssexual and romatic attraction
Assuyned normal parts
- Made her deel most comfortable, and default personality
- Anxiety withile switching,
Treatment
- Six months long
- Psychotherapy with cognitive behavioural therapy addressing stress and substance use disorder
- Happened aking with drug treatment to calm her down
- She was prescibred escitalopram to help reduce anxiety symptoms
- Her condition did not drasticallu change, meaning she still had the personalities, but her stress did get better.
Jeni HAynes (all from bbc)Linda/Maggot, a tall slender woman, “in a 1950s skirt with pink poodle appliqués, hair in an elegant bun with tapered eyebrows “. She gave a testimony to the academic and social impacts of Jeni’s abuse. She sought justice in 2009, but it was another 10 uears for the police to investigate. In my own opinion enis case is a good example of ritual abuse, as she say the abuse was “very calculated and precise, while still being extremely sadistic and extreme”, and the abuse was both sexual and physical, but since she had one abuser hers is a special case.
- Sshe was repeatedly raped and turtored by her father (richard haynes)
- She devlped 2500 distinct personalitiues to cope
- Six of her alters were allowed testify against him
- He was sentenced to 45 years in jail, starting at age 74, set to end when he was 121
- For most of hger early chuldhgood she was symphony, one of her algiers who was 4 years old, and she says that richard was abusing symphony, not jeni
- Symphony waas her first identity
- "She suffered every minute of Dad's abuse and when he abused me, his daughter Jeni, he was actually abusing Symphony," said by JEni
- Each identity in this complex coping strategy was speccifacy made to help her cope with each element of the abuse to keep her self alive
- The abuse was so bad that during the trial where 6 of jenis identities testify=ued,one of which was symphony, the only person who could be present was the judge, because the the case was too traumatizing for the jury
- After they told detailed accountants of every thing that happened, he was found guilty on 367 charges, including multiple accountants if rape, buggery, indecent assualt, and catnal knowledge of a child under the age of 10
- The abuse lasted 7 years, ending when she was 10 (when her parents divorced and she moved)
- Symphony gave particulars of the abuse,
- Muscles gave physical evidence,
- And linda testiied on the effects on jenis schooling and relationships
- She sought justice in 2009, but t took 10 years for the police to investigate
- Her mother was very supportive after learning about the abuse in 1984, and jeni said taht she beleives taht no one, not even her mother, was aware of the abuse
- Jeni also says that the abuse was very calculated and precise, while stillbeing extremely sadistic and extreme, as well as sexual and pyscial, making it what i think is a good example of DID caused by familial ritual abuse, but since it was one abuser it may not qualify
- The judge who sentenvced richard haynes, Judge SArah Huggett said that he would likely die in jail, she also called his crimes "profoundly disturbing and perverted" and "completely abhorrent and appalling", and said that it was “impossible” for the sentence to reflect the gravity of the harm
- DID saved jenis life, she even says so, as it has many other victims
"I passionately want my story told," Jeni told the BBC before the sentencing. "I want my 10-year struggle for justice to literally have been the fire that ripped through the field so that people behind me have a much easier road. "If you have MPD as a result of abuse, justice is now possible. You can go to the police and tell and be believed. Your diagnosis is no longer a barrier to justice." Both quotes from jenui
Imapct
- She is also unable to have a jpb and her and hermother live together off of government funded ch\ecks
- During her victim impact statment, jeni says;
- "spend our lives being wary, constantly on guard. We have to hide our multiplicity and strive for a consistency in behaviour, attitude, conversation and beliefs which is often impossible. Having 2,500 different voices, opinions and attitudes is extremely hard to manage".
- "I should not have to live like this. Make no mistake, my dad caused my Multiple Personality Disorder
Her identity
- Muscles - a n 18 year old styled like billy idol, who us tall and likes wearing clothes to show off his strong arms, he is calm and protective
- Volcano - verytall and strong, clad from top to toe in black leather with bleach blond hair
- Ricky - 8 years old but wears an old grey suit, with short bright red hair
- Judas short with red hair, 9plain grey school trousers, and bright green jumper, always looking as if hes about to speak
- Linda/maggot - tall, slender, in a 1950s skirt with pink poodle appliqués, hair in an elegant bun with tapered eyebrows
- Rick - wears huge glasses kuje those that richard haynes used to wear
Treatment
- Most treatment is pycchotherapy (aka talk therapy) which can help you understand why you dissociate abd give you tools to cope
- Other treatments include medication for co-occuriing issues
- Treatment cant make did go away, but it can help you cope with and reduce DID symptoms
Can you give yourself DID
- Did is created through extensive and intense child abuse, so unless you have that its a definite no
- If you developed did or the foundation of did as a child, it is possible to continue it onto adulthood
- If you did not develop did as a child, then no its not possible to make it during adulthood
- It also has a severe impact on peoples lives, and it is a bad one
Differences between identities
iidentity=ies can have different
- Medical histories,
- Abilities,
- Thought processes,
- Memoires,
- Knowledge,
- Perceived ages
- Perceived ethnicities,
- Perceived physical differences,
- Perceived ages,
- Perceived genders,
- Styles,
- Personalities,
- Likes and dislikes,
- sexual/romantic attraction
Basically everything that makes you you expect for your body
Method - using my research, i will come up with a list of symptoms to attempt to fix in order to create a more intensive treatment plan for DID. THis will be through research on symtoms causes and and possibke solutions
- Review data regarding symptoms
- Research bout the condition
- Research affect, on those with DID, HC, and A/MD
- Research causes on those with DID, HC, and A/MD
- Research currently used treatments and how they work
- Explain who they could or coudlnt work for those with DID
- Research possible un explored treatmentsj
Neurological symptoms
Negative correlation with hippocampus volume
The hippocampus is responsible for memory, short-term and long-term, and environmental awareness. The hippocampus organises, stores and retrieves your memories. Damage to the hippocampus can result in alzheimer’s disease, amnesia, dementia, encephalitis, epilepsy, hypoxia, post-traumatic stress disorder, and schizophrenia. Symptoms of damage to the hippocampus include memory loss, mood changes, and seizures. (9) Smaller hippocamal volumes were recorded in those with DID and PTSD, though the relationship between region-specific hippocamal volume reductions and dissociative symptoms/childhood trauma is still unknown. The hippocampal global volume was 6.75 % smaller on the left side of the brain and 8.33% smaller on the right side of the brain in the outpatients than in the healthy controls. In those with DID-PTSD, the left side was 10.19% smaller and 11.37% smaller on the right side compared to HC. (8)
Base
Function
The two most-influential theories for hippocampal function are related to space and memory. The spatial hypothesis was supported by the seminal discovery in 1971 of cells in the hippocampus that fired bursts of action potentials when a rat traversed specific locations in space, or “place fields.” That suggested that the hippocampus was a sort of device used by the brain for mapping layouts of the environment. Data supporting that idea came from later virtual navigation studies in humans, which suggested a strong association between the hippocampus and spatial navigation. The memory hypothesis originated in 1957 and was supported by studies and observations in which hippocampal removal resulted in a loss of the ability to form new memories, particularly fact- and event-related (declarative) memories. The two most influential theories
- Spatial hypothesis (space)
- Supported by seminar discover circa 1971 of cells in hippocampus that “fired bursts of action potentials when a rat traversed specific locations in space, or “place fields”
- This suggests that the hippocampus is used by the brain to map layouts of environments..
- More supporting data; virtual navigation study in humans, suggesting a strong connection between the hippocampus and spatial navigation in humans
- Memory hypothesis
- Originated in in 1957 supported by studies and observations in which the hippocampal removal resulted in a loss of ability to form new memories, specifically fact- and event-related (declarative) memories
- HPC importance to memory is indisputable, but the nature of the relationship is left to discussion
- Common theories
- binds items and contents to unified experiences and stores them
- Preferentially involved in conscious recollection or the experience f menta time travel duing recall
- Support rapid learning by reducing interference among similar memoriesmany think of it as an indexbinding elements of an experience but not storing mempies
Although there is near universal agreement among scientists that the hippocampus is important for memory, the exact processes by which the hippocampus supports memory are subject to much debate. Some studies suggest that the hippocampus binds items and contexts into unified experiences and stores them. Other studies suggest that the hippocampus is preferentially involved in conscious recollection, or the experience of mental time travel during recall. Still other studies suggest that the hippocampus is able to support rapid learning by reducing interference among similar memories (for example, where a person parked his or her car today versus yesterday). Some theories of hippocampal function treat the hippocampus as an index (much like an index at the end of a book) that binds together elements of an experience but does not store the experience itself. The latter is assumed to be stored in a distributed fashion throughout the brain, while the hippocampus is assumed to possess an index of that distributed code.
There is disagreement about whether long-term memories eventually become independent of the hippocampus, with the cortex being sufficiently able to support recall. That is known as the standard model of systems consolidation. The major competing theory, multiple trace theory, suggests that the hippocampus continues to be needed for long-term recall of episodic (context-rich) memories but not for semantic or gist memories. Finally, hippocampal structure, function, and connectivity are not uniform along its longitudinal axis. The anterior hippocampus is preferentially connected to the amygdala and orbitofrontal cortex and is thought to be involved principally in the regulation of emotion and stress. The posterior hippocampus is preferentially connected to the retrosplenial and posterior parietal cortices and is thought to be involved principally in cognitive and spatial processing.
Debatable on whether long term memories eventually become dependent on hippo campus, with occtrex able to support recall (standard model of systems consolidation. Major competeig theory = multiple trace theiry, hippocampus is needed episodic (context rich) memories, but not semantic/gist memories
Dysfunction
- One of the first studies of hippocampal dysfunction was patient Henry Maolaison (h.m)
- Underwent surgical removal of portons of medial temporal lobes including hippocampus and surrounding regions 1953 in an attempt to cure him of epiletic seizures
- After surgery his cognitice function stayed intact, however he lost his ability to create new declarative memories (this condition is anterograde amnesia, a common form of amnesia in patients with hippocampal dysfuction
- In alzehemiers, the hippocampus undergoes massive cell lose, connected with memory deficits manifested in early stages of the disease
- . Stress and depression are associated with a loss of ability to generate new cells in the dentate gyrus, as well as a loss of dendritic spines and reduced dendritic branching throughout the hippocampus. Hippocampal dysfunction is also implicated in schizophrenia and associated disorders, suggesting that that region of the brain is particularly vulnerable to neuropsychiatric disease
- The hippocampus often is the focus of epileptic seizures, which can lead to hippocampal sclerosis (a pathological loss of hippocampal cells..
The hippocampus is an area of focus for treating; damage to declarative memory (anterograde amnesia), overall memory (look at connections between the hippocampus in alzehemiers and DID), correlations between hippocampal dysfunction and neuropsyciatric disease (mentioned stress, depression, schizophrenia (and associated dsorders)), and epilesy (unexplained neurological symptoms) One of the earliest studies of hippocampal dysfunction was that of “patient H.M.” (Henry Molaison), who in 1953 underwent surgical removal of portions of the medial temporal lobes, including removal of the hippocampus and surrounding regions, in an attempt to cure him of epileptic seizures. Following the surgery, his cognitive functions were mostly intact; however, he lost the ability to create new memories for facts and events, a condition known as anterograde amnesia. Such amnesia is typical in disorders that involve hippocampal dysfunction. For example, in Alzheimer disease, the hippocampus undergoes massive cell loss, which is associated with memory deficits that manifest in early stages of the disease. Stress and depression are associated with a loss of ability to generate new cells in the dentate gyrus, as well as a loss of dendritic spines and reduced dendritic branching throughout the hippocampus. Hippocampal dysfunction is also implicated in schizophrenia and associated disorders, suggesting that that region of the brain is particularly vulnerable to neuropsychiatric disease. Individuals who survive a hypoxic episode (temporary deprivation of oxygen in the brain) often sustain hippocampal damage and anterograde amnesia. Finally, the hippocampus often is the focus of epileptic seizures, which can lead to hippocampal sclerosis (a pathological loss of hippocampal cells).
Anterograde amnesia
 overall
overall-
Overlaps with DID
-
Treatment plan
LOss in the ability to foorm new memories, siemethin that has not yet come up inmy research. Hippocampal dysfunction can lead to anterograde amnesia Posttraumatic anmesia (PTA) (can be retrograde or anterograde) Look into brain damage in concussion and overlaps with DID
Alzehmeirs
In early stages of AD, we observe rapid loss of tissue in the hippocampus, similar to the decrease in hippocampal tiswsue observed in mature cases of DID. This rapid loss of hippocampal tissue in early stages of AD is associated functional dissocoection with other areas of the brain. A lack of siruin (SIRT) expression in the hippocampal neurons impair cognitive function, Proliferation, differenttion, anf migrations are stes involved in adult neurogenesis. The microglia in the hippocampal region are more immunologically active than the other regions of the brain.
In the early stages of AD, the hippocampus shows rapid loss of its tissue, which is associated with the functional disconnection with other parts of the brain. ) n the progression of AD, atrophy of medial temporal and hippocampal regions are the structural markers in magnetic resonance imaging (MRI). Lack of sirtuin (SIRT) expression in the hippocampal neurons will impair cognitive function, including recent memory and spatial learning. Proliferation, differentiation, and migrations are the steps involved in adult neurogenesis. (3) The cerebral cortex and hippocampus are closely associated with cognitive function and neurogenesis in the brain Seeing a lot of connections between neuroanatomy with DID and AD Along with the β-amyloid and tau proteins, trans-active response deoxyribonucleic acid (TAR DNA)-binding protein of 43 kDa (TDP-43) is also a newly linked protein in the AD. TDP-43 protein accumulates in the amygdala and spreads into the hippocampus, leading to faster atrophy (Josephs et al. 2017). Hence, prevention of spreading this protein into the hippocampus could treat AD Treatment possibility - genetic nueroimagining works showed - ad risk alleles show curcilial role in cortical and hippocampal morphometry The genetic neuroimaging works have proved that the AD risk alleles show a crucial role in cortical and hippocampal morphometry (Lancaster et al. 2019). In AD, neuronal degeneration happens because of the accumulation of two abnormal proteins, β-amyloid, and tau, in the brain. The characteristic feature of AD is an excessive formation or decreased elimination of amyloid-beta (Aβ). Microscopically and pathologically, AD is described as the extracellular accumulation of senile plaques in addition to the intracellular accumulation of the neurofibrillary tangles in various parts of the brain, particularly in the hippocampu How much is DID a neurological issue? Nuerological changes in hippocampus If i remember correct, there was hyper arousal in amygdala as a stress reposnse inthose with PTSD Though hippocampal degeneration is also seen in other neurodegenerative diseases like Lewi body dementia, the degree of deterioration is markedly more in AD. The knowledge of variation in the hippocampus will help diagnose and treat AD (Elder et al. 2017). The patients with AD are clinically presented with the deterioration of activity of daily living due to the cognitive and functional decline The hippocampal sub-regions aid in the process of the generation of episodic memory Episodes are one symptom of PTSD/trauma, alters who have episodes vs ones who have no memories Is DID a neurodegenerative disease? Repressed memories The nerve growth factor (NGF), neurotrophin 3 (NT-3), neurotrophin 4/5 (NT-4/5), and the brain-derived neurotrophic factor (BDNF) are the proteins, which specifically help the survival of neurons in AD patients (Hock et al. 2000). BDNF is one of the significant neurotrophins, which protect the neurons by promoting their survival against the various neuronal insults in different brain regions, including the hippocampus (Rai et al. 2013). The primary source for the BDNF is the neuron. Apart from the neurons, astrocytes and microglia also contain the BDNF (Lisman et al. 2017). The oxidative stress can reduce the BDNF expression, thereby leading to hippocampal atrophy. Therefore, antioxidants can reduce oxidative damage, which occurs due to the oxidative stress. It was reported that levels of ratios of NT-4/NT-3, NT-4/NT-5, and BDNF had been considerably declined at the hippocampus of AD models (Hock et al. 2000). However, the intensities of NGF/NT-3 ratio and NGF were increased at the hippocampus of AD animal models. Hocket al. (2000) suggested that declined intensities of the BDNF might lead to neuronal degeneration in AD. It was reported that NGF and BDNF had protected the basal forebrain cholinergic neurons from the degeneration, which was induced by the axotomy (Knusel et al. 1992). Along with this, neurons containing 5-hydroxytryptamine are also decreased in the brain, which causes depression and behavioral changes in AD (Raskind and Peskind 1994). The process of neurogenesis The neurogenesis occurs at the niche, where the neural stem cells (NSCs) are seen near the blood vessels. The signals from the neurons and blood vessels will influence the NSC proliferation and differentiation. Several animal experiments have shown that the systemic factors in the circulation positively influence brain neurogenesis. Ozek et al. (2018) observed that the administration of GDF 11 has improved the hippocampal vascular niche in old mice. They have also reported that systemic administration of GDF 11 has elevated the newborn neuron (Bromodeoxyuridine, BrdU+/ neuronal nuclear protein, NeuN+), neural stem cells (sex-determining region, Sox2+), and neural progenitor/immature neurons (doublecortin, DCX+). Ozek et al. (2018) observed that GDF 11 had improved the vasculature of the hippocampus by increasing the blood vessels and their branches. But these improvements were honored to be only seen in the old mice brains. Laack of neurogensis may be found in patients with DID Found a way to increase neurogenesis It was reported that, genetic activation of activing—like kinase 5 (ALK 5) receptor for the GDF 11, has improved the neurogenesis in hippocampus by activating the downstream signalling through spinal muscular atrophy (Sma-) and mothers against decapentaplegic (Mad-)-related proteins 2/3 (SMAD 2/3). Hence, GDF11 improves hippocampal neurogenesis and vasculature (Ozek et al. 2018). The GDF-11 is present in the bloodstream, with some of it crossing the blood–brain barrier (Ozek et al. 2018). It is believed to exhibit several beneficial effects on the vasculature by promoting angiogenesis, maintenance of blood–brain barrier and vascular stability (Sutherland et al. 2020). Aging will cause impaired neurogenesis due to the decreased vascular density and blood flow. The brain of elderly individuals is predisposed to many stressors, leading to irreversible brain damage. The recent trends suggest that GDF-11, which is present in young people's blood, can have neuroprotective effects (Lu et al. 2018). It was reported that the circulating GDF-11 in the blood decreases with the increasing age (Poggioli et al. 2016). This suggests that patients with AD may have reduced levels of GDF in their blood. NSCs have the self-renewal capacity and can differentiate into cells like neurons, oligodendrocytes, and astrocytes. The differentiated neurons help organize complex neuronal circuits, which are essential during the processing of information and transmission (Kino 2015). NSCs, after becoming the neuroglial cells like astrocytes and oligodendrocytes, will help in the proper functioning of neurons. DG of the hippocampus contains plenty of these NSCs (Androutsellis-Theotokis et al. 2008), which help in learning and memory. NSCs also increase the response to anti-depressant drugs and help in the subsequent recovery (Kino 2015). The adult NSCs in the hippocampus can grow and maintain their number throughout life (Zhang et al. 2015). NSCs are involved in consolidating, preserving, and organizing the memory, which is mediated by the hippocampus. They also assist in mood and behavioral integrity. Connecion between stem cells and stress. Specifically post traumtic/traumatic NSCs are involved in the turnover of pyramidal cells, which is important for replacing old memory traces with new ones. NSCs are described to have their capacity in neuronal regeneration. The NSC transplantation therapy is a favourable means of managing neuronal diseases and restoration of microenvironment at the injury site (Tang et al. 2017). They secrete soluble factors, which include cytokines, growth factors, and neurotrophic factors. These factors can protect the existing neurons against the damage in situ. AD is caused by neuronal or neuroglial cell defects, resulting in memory deterioration, cognitive disorders, dementia, and body movement disorders. (symptims or side effects of dissociation?) It was described that hippocampal neuronal mitochondria are decreased in AD patients. The transplantation of NSCs into the transgenic AD mice model has shown a significant increase in the mitochondrial number and expression of mitochondria-related proteins. This has improved the cognitive function in a mouse model (Zhang et al. 2020). Human NSCs have been tried to treat AD in transgenic animal models (Li et al. 2016; Blurton-Jones et al. 2014). It was reported that intranasal administration of NSCs showed the ability to migrate to different regions of the central nervous system, including the hippocampus, cerebral cortex and spinal cord (Zhang et al. 2020). Though most of the parts of the brain are affected in AD, the regions which are essential for the learning and memory like hippocampus, entorhinal cortex, and basal forebrain show marked degeneration. (research learning and did) Decreased neurotrophin expression and its impaired neuronal transport are apparent in the neurodegenerative brain. Hence, maintaining the regular neurotrophin expression can be a treatment modality in AD management. Marsh and Blurton-Jones (2017) have demonstrated the potential benefits of NSCs in providing neurotrophic support in AD. The lifestyle controls the human brain's function. Physical activity, food habits, and exposure to stress can impact the cognitive reserve of the brain. The animal model research has shown that running exercise can increase the hippocampal neurogenesis. The pro-neurogenic lifestyle will control the capability of the brain to prevent the neuronal degeneration due to the trauma, aging, and diseases (Valero et al. 2016). It was reported that, the low calorie diet and physical exercise can promote the adult neurogenesis. The omega-3 polyunsaturated fatty acids are required for the proper neuronal function as they exert an anti-inflammatory effect (Valero et al. 2016). It was reported that physical activity has prevented the decline of neurogenesis and boosted the memory in aged rodents and mouse AD models (van Praag 2008). Stress and severe exercise can elevate the glucocorticoids and affect the microglia (Gleeson et al. 2011). Both acute and chronic stresses decrease the adult neurogenesis due to the reduction in proliferation of neuroprogenitor cells and survival of newborn cells (Schoenfeld and Gould 2012). Animal research has shown that the high fatty diet has decreased the cell proliferation, cell survival and increased apoptosis in the DG (Park et al. 2011). It was observed that the high-fat diet decreased the BDNF and omega-3 polyunsaturated fatty acids increased it. This suggests that diet has a role in the maintenance of BDNF levels. Obesity and high-fat diet are associated with the state of chronic systemic inflammation, which increases the levels of pro-inflammatory cytokines like IL1-β and tumor necrosis factor α (TNFα) by the adipose tissue (Gregor and Hotamisligil 2011).
Stress and depression were mentioned in this specific research, and since shizophrenia wa sthe only other tat came up in hippocampal research and the overlapping symptoms are physcologiccal and not biologcal, thi is our most promising research thus far.
Grey matter volume
The grey matter in the brain makes up the outermost layer. Grey matter has a high neuron count, allowing for information processing and release. (11) Relative to HC, patients with DID and PTSD showedlower volumes of cortical grey matter throughout their whole brain, specifically in their frontal, temporal, and insular cortices. Comorbid patients showed larger pallidum volumes and larger putamen and pallidum volumes relative to patients with PTSD only. (10) (subcrtical and whole brain cortical)
We mainly see grey matter loss in the cerebral cortex and hippocampus
In this paper, we report findings from the largest meta-analysis conducted to date of VBM studies in MDD and BD. We compared results from these two conditions to identify common and distinct patterns of grey-matter volume alterations. We showed that the two conditions share similar patterns of lower volume in the bilateral insula and medial prefrontal cortex, suggesting that there may be an underlying pathological mechanism that is common to affective disorders. A number of regions, including the left hippocampus and right dorsolateral prefrontal cortex, differed between conditions, indicating that these disorders may be associated with spatially distinct patterns of pathophysiology.
Both conditions showed smaller grey-matter volumes relative to control groups in the medial prefrontal systems, including the anterior cingulate cortex. In MDD, this was predominantly located in the most ventral and dorsal regions of the medial prefrontal cortex, while in BD it was located in a large cluster anterior to the genu of the corpus callosum, although this difference in location was not statistically significant. The conjunction analysis indicated that the volumes of parts of the dorsomedial and ventromedial prefrontal cortex were robustly lower in both conditions, suggesting a consistent pattern across disorders. These regions have been strongly implicated in mood regulation, and the anterior cingulate cortex in particular has been shown to be crucial in the regulation of affective states,27 and has been a target of treatment with deep brain stimulation.28 Our results are consistent with theories of mood dysregulation in affective disorders that posit that dysfunction in regions such as the medial prefrontal cortex leads to aberrant mood states.29 Further work is necessary, however, to determine whether the structural differences here are responsible for the altered function of these networks.
We also found that bilateral insula volume was smaller in patents in both conditions. This region is involved in a range of functions, including affective processing and awareness of bodily states,30, 31 and atypical functioning of this region in affective disorders has been found in functional neuroimaging research.32, 33 Notably, the insula has also been found by multiple studies to predict treatment response in patients with depression.34, 35 Our finding of smaller insular volume in both unipolar and bipolar subjects suggests that structural abnormalities are present in the same areas in which altered function has also been identified. The insula has been implicated in interoceptive processing and general bodily awareness,36 and our results may indicate that structural changes are associated with altered interoceptive function in affective disorders;37, 38 this is a speculative interpretation, however, that requires direct testing.
Our comparison of the conditions revealed several areas of smaller grey-matter volume that were significantly greater in MDD than in BD, most prominently in the left parahippocampal gyrus and right dorsolateral prefrontal cortex, specifically the middle frontal gyrus. Smaller volumes of the hippocampus and parahippocampal gyrus have been well documented in MDD, but have been reported less often in BD.12, 14, 39 Investigators have suggested that this may be due to neuroprotective effects of lithium, which counteracts volume loss in BD.40 We did not find any significant heterogeneity in the hippocampus in BD, suggesting that there was no variation in effect sizes due to medication or other variables. It is important to note, however, that we cannot exclude the possibility that this may be due to reduced sensitivity of whole-brain VBM analyses in small regions such as the hippocampus.41 Additionally, it is unlikely that this difference between conditions can be explained by mood state in MDD given that our meta-regressions showed that lower depression severity in MDD was associated with smaller volumes in this region. Alternatively, this may reflect sparing of the hippocampus in BD due to protective factors in individuals predisposed to the disorder.42
The dorsolateral prefrontal cortex has been linked to emotion regulation,43 and the right dorsolateral prefrontal cortex specifically has been associated with attentional control during emotional tasks.44 Notably, repetitive transcranial magnetic stimulation to this region has been reported to improve symptoms in treatment-resistant depression,45 but results have been less convincing in bipolar depression.46 Our findings add to this literature by suggesting that volumetric alterations in this region are specific to MDD, indicating that a differential pattern of prefrontal grey-matter volume may potentially differentiate these two disorders. It is important to mention that functional alterations have been identified in the right dorsolateral prefrontal cortex in BD.47 The relationship between functional and structural alterations in these conditions remains unclear; and further research is essential to understand potential functional and/or structural disease-specific alterations within affective disorders in the dorsolateral prefrontal cortex.
Our analyses within each condition also revealed a number of areas of grey-matter changes that did not differ significantly in magnitude between disorders but that were not reliably smaller in both disorders relative to controls. One notable difference in MDD compared with controls involved the bilateral occipital cortex, including primary visual and extrastriate cortices, where patients showed a large area of greater volume relative to controls. Although a number of studies have highlighted the possibility of neurochemical48 and functional49, 50 changes in these regions, we believe this is the first study to identify robust volumetric changes in these locations. Given our efforts to ensure that our results were reliable and robust, it is unlikely that this is simply a false positive produced by the meta-analytic method, although we cannot exclude the possibility that methodological issues in the original studies may have caused spurious results. For example, it is possible this could be an artefact caused by correction for intracranial or total grey-matter volume combined with substantially lower grey-matter volume in other areas, although this is a speculative interpretation and would require confirmation. The potential role of occipital regions has rarely been investigated in major depression, and further research is required to understand whether these results are robust or whether they are a result of the method used.
We found a number of regions that showed significant between-study heterogeneity, and we explored these using meta-regressions. In MDD, studies with less severely depressed patients showed smaller grey-matter volume in the hippocampus than did investigations with more severe patients. This may seem contradictory given that previous studies have showed the opposite pattern.51, 52 It is possible that it may be explained by the use of medication. Treatment with selective serotonin reuptake inhibitors is known to increase hippocampal volume,53, 54 and given this it is possible that more severely depressed patients had received more extensive pharmacotherapy in the past, leading to amelioration of pre-existing grey-matter volumetric abnormalities, although we were unable to test this here due to historical treatment data being unavailable in the original studies. However, it is important to note that we only had access to information regarding current depression severity, and it is possible that lifetime depression severity, or chronic and treatment-resistant symptom profiles, may be associated with different neuroanatomical profiles.
Our meta-regression analyses showed effects of demographic variables in both conditions. In MDD, volume of the prefrontal cortex was smaller in studies with fewer male patients. Anatomical differences between sexes have been reported previously in depression,55 although it is unclear what drives these differences. In addition, we found smaller left insula volumes in studies of MDD with older patients; in contrast, in BD studies with older patients, we found smaller volumes in the right middle temporal gyrus. Thus, there may be a different biological trajectory in affective disorders in relation to these regions, although meta-regressions should be interpreted with caution as they do not directly test relations within samples.
This meta-analysis improves on previous studies in several ways. First, the novel meta-analytic method used here allowed us to identify common and distinct areas of grey-matter volume alterations in affective disorders. Given the paucity of reports comparing affective conditions directly, this approach enabled us to identify volumetric aspects of common neuropathological mechanisms, and potentially distinctive biomarkers. Second, we were able to include a larger number of studies due to the rapid growth of the field and our access to as-yet unpublished data sets. We are therefore able to provide the most conclusive picture of volumetric changes currently available. Third, we included a number of original statistical maps in our analyses. This substantially improves the sensitivity and specificity of the analysis, especially in cases in which individual studies have small samples.19 Finally, the thorough and detailed approach used in this work ensured that findings were robust and that heterogeneity was comprehensively explored. We found no evidence of publication bias or small-study effects; nevertheless, it is important to note that, given the small sample sizes of the majority of the studies included in the analyses, we cannot exclude the possibility of small-study bias.
Despite these strengths, we should also note several limitations of this meta-analysis. First, we cannot determine causality from these results due to the fact that all the included studies were cross-sectional group comparisons, and it is not clear whether these alterations are part of the pathogenesis of these disorders or a consequence of the illness. It should be noted however that our meta-regressions did not detect any effect of illness duration, providing some evidence against the latter explanation. Second, the effect size comparisons may not provide as accurate a picture of group differences as studies directly comparing the two conditions. To date, there have been very few VBM studies directly comparing affective conditions15, 16 making it difficult to draw firm conclusions concerning potential similarities and differences between disorders. Hence, at present, the approach used in this meta-analysis, with the limitation of indirectly comparing studies’ effect sizes, offers the most viable option to reach conclusions generalisable beyond individual studies. Additionally, given the inherent robustness of the meta-analytic method, our results should provide a summary of the most reliable differences between these disorders.
Third, the samples used in the studies differed between disorders with respect to treatment status (for example, different types of pharmacotherapy). Given that psychotropic medications can have effects on brain structure,53 it is difficult to be certain that results are not entirely independent from medication status. As a related point, the samples also differed in mood state and illness duration. We found no evidence for effects of these variables in meta-regressions within disorders, suggesting that this is not likely to be a major concern. However, effects of mood state are particularly difficult to rule out, given that a number of studies included samples of mixed mood states and several did not provide information on mood state. Consequently, it is not possible to comment with certainty on the effect of mood state on our results. Furthermore, we cannot exclude the possibility that undiagnosed cases of BD presented as unipolar depression in the original studies,6 and it is not possible to rule out the influence of comorbidities such as anxiety disorders on the results as these were not always well described in the original reports. Another concern is that many of the retrieved studies included more controls than patients. Although these unbalanced studies may have theoretically biased results,56 it is not clear from the existing literature that this is likely to affect our findings and conclusions.
Finally, we cannot be certain that these regions of common grey-matter volume alterations are exclusive to affective disorders. A recent meta-analysis by Goodkind et al.57 found that some of these areas, such as the insula and dorsomedial prefrontal cortex, are lower in volume across a range of psychiatric conditions including affective, anxiety and psychotic disorders. This suggests that morphometric grey-matter changes in these regions are not specifically pathognomonic to affective disorders, or are even a proxy for underlying common disease processes or for risk factors such as life stressors or effects of hormonal or inflammatory changes. Nevertheless, the locations identified by Goodkind et al. differ from those reported in this meta-analysis in their location and size. For example, the authors demonstrated that the anterior left insula extending to the left inferior frontal gyrus was affected across disorders. In our work, a more posterior portion of the left insula was shown to be affected in both MDD and BD, which has functional relevance given the anterior-posterior division in insula function, with the posterior region being specifically involved in interoception and bodily awareness.36
In conclusion, we have shown that MDD and BD show a common pattern of lower grey-matter volume which predominantly includes the medial prefrontal and insular cortices. In addition, the two conditions also show distinct patterns of volume alterations in a number of other regions, most predominantly the right dorsolateral prefrontal cortex and left hippocampus, which are specific to MDD. There is significant heterogeneity within these results, but this could be partially explained by clinical and demographic differences in clinical samples. These findings suggest targets for neuroanatomical diagnostic biomarkers, but also indicate that affective disorders are more morphologically similar than they are different.
White matter
White matter is brain matter found within the deep tissues of the brain. It has axons, extensions of neurons, that are often covered in Mylelin, giving it that white colour. White matter conducts, processes, and sends nerves signal up and down the spinal cord. (12, 13) All participants underwent DTI, diffusion tensor imaging, to measure the white matter in their brains. (14) Patients with DID showed reduced white matter in their bilateral pallidum, midbrain, and pontocerebellar white matter. (14)
Unexplained symptoms
Unexplained neurological symptoms are especially prevalent in DID. These include non-epileptic seizures, paralysis/sensory loss, and unexplained bodily sensations while switching. (15)
Non epileptic seizures (5)
Psychogenic nonepileptic seizures are episodes of movement, sensation, or behaviors that are similar to epileptic seizures but do not have a neurologic origin; rather, they are somatic manifestations of psychologic distress. Patients with psychogenic nonepileptic seizures frequently are misdiagnosed and treated for epilepsy. Video-electroencephalography monitoring is preferred for diagnosis. From 5 to 10 percent of outpatient epilepsy patients and 20 to 40 percent of inpatient epilepsy patients have psychogenic nonepileptic seizures. These patients inevitably have comorbid psychiatric illnesses, most commonly depression, posttraumatic stress disorder, other dissociative and somatoform disorders, and personality pathology, especially borderline personality type. Many patients have a history of sexual or physical abuse. Between 75 and 85 percent of patients with psychogenic nonepileptic seizures are women. Psychogenic nonepileptic seizures typically begin in young adulthood. Treatment involves discontinuation of antiepileptic drugs in patients without concurrent epilepsy and referral for appropriate psychiatric care. More studies are needed to determine the best treatment modalities.
Patients have comorbid psychiatric illness, noteably depression, PTSD, somotaform disorders, dissociative disorders, and often have a traumatic hustory of sexual and phsycial abuse Nonepileptic seizures are involuntary episodes of movement, sensation, or behaviors (e.g., vocalizations, crying, other expressions of emotion) that do not result from abnormal cortical discharges. The seizures can mimic any kind of epileptic seizure and thus can be mistaken for generalized tonicclonic seizure, absence seizure, and simple or complex partial seizures.1 Early recognition and appropriate treatment of nonepileptic seizures can prevent significant iatrogenic harm and may result in a better outcome. Irsk factors include anxiety disorders (PTSD) dissociative disorder (DID), and somatization disorder Risk factors Psychogenic Misinterpretation of physical symptoms Psychopathologic processes Anxiety disorders, including posttraumatic stress disorder Conversion disorder Dissociative disorders Hypochondriasis Psychoses Somatization disorders Reinforced behavior patterns in cognitively impaired patients Response to acute stress without evidence of psychopathology Physiologic Cardiac arrhythmias Complicated migraines Dysautonomia Effects of drugs and toxins Hypoglycemia Movement disorders Panic attacks Sleep disorders Syncopal episodes Transient ischemic attacks Vestibular symptoms
Psychogenic nonepileptic seizures are a physical manifestation of psychologic distress. They are grouped into the category of psychoneurologic illnesses (e.g., conversion disorder, somatization disorders), in which symptoms are psychiatric in origin but neurologic in expression.5 This article focuses on psychogenic nonepileptic seizures. Psychogenic nonepileptic seizures are a physical manifestation of psychologic distress. They are grouped into the category of psychoneurologic illnesses (e.g., conversion disorder, somatization disorders), in which symptoms are psychiatric in origin but neurologic in expression
The presence or absence of self-injury and incontinence, the ability to induce seizures by suggestion, psychologic tests, historical factors, and ambulatory electroencephalography (EEG) have been found to be insufficient for the diagnosis of psychogenic nonepileptic seizures.1,6 Postictal prolactin levels greater than two times the upper limit of normal once were thought to differentiate generalized and complex partial seizures from psychogenic nonepileptic seizures but recently have been shown to be unreliable.7
All psychogenic nonepileptic seizures function as a coping mechanism.23 Patients with these events are more likely to use maladaptive coping strategies to handle stress.24 In psychogenic nonepileptic seizures, psychologic conflicts are translated into a physical symptom—the seizure. In this way, intolerable distress is dissociated from the painful conscious experience of the trauma or forbidden emotions that are causing the distress.25,26 Thus, genuine psychogenic nonepileptic seizures (as opposed to factitious disorder or malingering) are not intentional: they are created as a psychologic defense mechanism to keep internal stressors out of conscious awareness.25 All pyscogenic non epileptic function as a coping mechanism, patients are more likely to use maldaptive coping mechanisms for stress, intolerable distress is dissociated from the painful conscious experience of the trauma or forbidden emotions that are causing the distress Psychogenic nonepileptic seizures do not have a single etiology; rather, they are the product of several different causal pathways (Table 1). The seizures may be the result of psychopathologic processes, a response to acute stress in patients without evidence of psychopathology, or a reinforced behavior pattern in cognitively impaired patients. Rarely, malingering or factitious disorder presents as psychogenic nonepileptic seizures.27
From 43 to 100 percent (median: 73.5 percent) of patients with psychogenic nonepileptic seizures have concurrent psychiatric disorders28 (Table 3).25 The disorders tend to be related to trauma, and include posttraumatic stress disorder (PTSD) and other anxiety disorders; depressive disorders; and conversion, somatization, and dissociation disorders. Personality pathology, particularly of the borderline type, is common.29 Frequently, patients with psychogenic non-epileptic seizures also have other dissociative and somatization symptoms.18,30 Patients with psychogenic nonepileptic seizures frequently have a history of (or current) physical or sexual abuse24 or significant psychosocial stressors for which there is no perceived resolution.31,32 These “unspeakable dilemmas”31 often involve dysfunctional family interaction and communication.18,24
A frequently cited prospective study25 showed that 84 percent of patients with psychogenic nonepileptic seizures had experienced trauma. One recent study33 found significantly higher rates of PTSD, childhood sexual abuse, dissociative symptoms, and history of assaultive trauma in patients with psychogenic nonepileptic seizures than in patients with epilepsy. Physical and sexual abuse has been linked to increased rates of several somatization syndromes, including psychogenic nonepileptic seizures.26 Disorders tend to be related to trauma, (PTSD, DID, prespression, anxiety disorders, somatization) Patients with psychogenic nonepileptic seizures frequently have a history of (or current) physical or sexual abuse One recent study33 found significantly higher rates of PTSD, childhood sexual abuse, dissociative symptoms, and history of assaultive trauma in patients with psychogenic nonepileptic seizures than in patients with epilepsy. Physical and sexual abuse has been linked to increased rates of several somatization syndromes, including psychogenic nonepileptic seizures 84% of patents with psycogenic non epliletic disorders have traumatic history To determine why a patient is having psychogenic nonepileptic seizures, the physician must identify the psychologic function of the seizure.34 A detailed, systematic psychiatric evaluation and an assessment of family, social, financial, and employment problems should provide insight.35 Causes and suggested treatments for psychogenic nonepileptic seizures are summarized in Table 4.3,9,25,27,35,36
PTSD/Dissociation
The patient has active chronic PTSD and dissociative symptoms. Flashbacks, recollections, or sensory triggers often initiate psychogenic nonepileptic seizures. Often, there is a history of severe childhood or current abuse. Exposure-based therapies and selective serotonin reuptake inhibitors for PTSD
No randomized controlled studies have been conducted on the treatment of psychogenic nonepileptic seizures.27,28 Treatment recommendations are based on the theory that because the seizures are psychogenic in origin, they will respond to psychiatric treatment. Two uncontrolled studies18,39 have shown that psychotherapy is more effective than no intervention.
Various psychotherapeutic techniques with proven efficacy in other disorders have been applied to patients with psychogenic nonepileptic seizures who have similar psychiatric profiles. Table 43,9,25,27,35,36 summarizes current treatment recommendations based on the underlying causes of psychogenic nonepileptic seizures. All recommendations are based on anecdotal evidence or small, uncontrolled studies.
In one model,27 the first step is accurate diagnosis of psychogenic nonepileptic seizures based on a thorough history, a focused physical examination, and inpatient vEEG monitoring. After the diagnosis is presented to the patient and family, the next step is to create a list of predisposing factors, precipitants, and perpetuating factors for the seizures. This list is used to determine the appropriate psychotherapies and drug treatments. Antiepileptic drugs are tapered in patients with exclusively nonepileptic seizures, and appropriate psychotropic drugs are titrated for the treatment of psychiatric comorbidities.
Phsycobiological symptoms symptoms
They also show psychobiological changes between alters, with differences in: “vision, medication responses, allergies, plasma glucose levels in diabetic patients, heart rate, blood pressure readings, galvanic skin response, muscle tension, laterality, immune function, EEG readings” (Dissociative identity disorder (DID) DSM5 code 300.14 (ICD-10 F44.81)) SDID patients function as two + identity sates (DIS), NIS (nuetreal identity state), and TIS traumatic identity state NIS inhibit inhibit access to traumatic history, allowung for higher functioning TIS has access to traumatic history and responses This is testing to see psycobiologic changes between DI (6) Dissociative identity disorder (DID) patients function as two or more identities or dissociative identity states (DIS), categorized as ‘neutral identity states’ (NIS) and ‘traumatic identity states’ (TIS). NIS inhibit access to traumatic memories thereby enabling daily life functioning. TIS have access and responses to these memories. We tested whether these DIS show different psychobiological reactions to trauma-related memory. Methods A symptom provocation paradigm with 11 DID patients was used in a two-by-two factorial design setting. Both NIS and TIS were exposed to a neutral and a trauma-related memory script. Three psychobiological parameters were tested: subjective ratings (emotional and sensori-motor), cardiovascular responses (heart rate, blood pressure, heart rate variability) and regional cerebral blood flow as determined with H215O positron emission tomography. Tested methods, subjectibe ratings (emotional and sensorimotor), cardiovascular responses (heart rate, blood pressure, heart rate bariability), and reginal cerebral blood flow a determined with H215O postrion emssion Results Psychobiological differences were found for the different DIS. Subjective and cardiovascular reactions revealed significant main and interactions effects. Regional cerebral blood flow data revealed different neural networks to be associated with different processing of the neutral and trauma-related memory script by NIS and TIS. Conclusions Patients with DID encompass at least two different DIS. These identities involve different subjective reactions, cardiovascular responses and cerebral activation patterns to a trauma-related memory script.
(7) Abstract Dissociative identity disorder (DID) is a chronic post-traumatic disorder where developmentally stressful events in childhood, including abuse, emotional neglect, disturbed attachment, and boundary violations are central and typical etiological factors. Familial, societal, and cultural factors may give rise to the trauma and/or they may influence the expression of DID. Memory and the construction of self-identity are cognitive processes that appear markedly and centrally disrupted in DID and are related to its etiology. Enduring decoupling of psychological modes may create separate senses of self, and metamemory processes may be involved in interidentity amnesia. Neurobiological differences have been demonstrated between dissociative identities within patients with DID and between patients with DID and controls. Given the current evidence, DID as a diagnostic entity cannot be explained as a phenomenon created by iatrogenic influences, suggestibility, malingering, or social role-taking. On the contrary, DID is an empirically robust chronic psychiatric disorder based on neurobiological, cognitive, and interpersonal non-integration as a response to unbearable stress. While current evidence is sufficient to firmly establish this etiological stance, given the wide opportunities for innovative research, the disorder is still understudied. Comparison of well-selected samples of DID patients with non-dissociative subjects who have other psychiatric disorders would further delineate the neurobiological and cognitive features of the disorder, whereas genetic research on DID would further illuminate the interaction of the individual with environmental stress. As such, DID may be seen as an exemplary disease model of the biopsychosocial paradigm in psychiatry.
Studies conducted in various countries led to a consensus about prevalences of DID:Citation3 5% among psychiatric inpatients, 2–3% among outpatients, and 1% in the general population. Prevalences appear heightened among adolescent psychiatric outpatients and in the psychiatric emergency unit.Citation4,Citation5 The latter points to the acute transient crisis situations that may be superimposed on an underlying DID. Such crises usually serve as a diagnostic window for the clinician in conditions when core symptoms of DID remain dormant until a stressful event triggers a more prominent manifestation.
Self-report instruments such as the Dissociative Experiences Scale (DES),Citation6 the Dissociation Questionnaire (DIS-Q),Citation7 and the Multidimensional Inventory of Dissociation (MID)Citation8 serve as potential screening measures for patients with DID. Clinician-administered instruments such as the Dissociative Disorders Interview Schedule (DDIS)Citation9 and the Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D)Citation10 guide the clinician in making a firm diagnosis of DID.
DID is a stable diagnostic category when the primary components of the disorder are considered: the existence of dissociative identities, confusion about and alterations between them, amnesia, and experiences of depersonalization and derealization.Citation11 The foundation of dissociative identities is thought to be divisions or dissociations within the individual at the level of identity or the personality. Dissociation or a breakdown of integration between psychobiological aspects and systems that make up the totality of the person’s functioning can occur at the level of sensation (e.g., temporary/functional blindness), cognition (e.g., amnesia), affect (e.g., numbing), behavior (e.g., temporary/functional paralysis), and consciousness (e.g., ego-observing depersonalization), among others.Citation12
Yet, when all these systems come together to underpin and maintain a person’s identity, and dissociation occurs at this (identity/personality) level, it creates dissociative identities. Here, separate organized systems of functioning, with their own unique perspective on the world and who they are, appear to co-exist within the individual.Citation13 Each of these identities has their own first-person perspective or experience of self-consciousness.Citation14–Citation16 Consequently, each of these identities reports their own subjective experiences and memories, their own sense of agency and will, and their own perspective on who they are.Citation14 They often report being unaware of other identities or report amnesia for experiences that presumably occurred when other identities were engaging in executive actions.
This paper examines the etiological factors of DID, setting them around the current most widely accepted primary driver of the psychopathology: developmental traumatization. Secondarily, family and sociocultural factors and further cognitive and neurobiological disturbances emerge in tandem with this primary factor. These etiological factors have also been the subject of an accumulating body of research in the field of dissociation in general and dissociative disorders other than DID. However, in this paper, only studies directly addressing DID have been considered for examination.
Developmental traumatization DID is currently understood as a chronic complex post-traumatic developmental disorder where adverse experiences usually begin in early childhood and in which the dissociative identities result from the child’s inability to develop and maintain a unified sense of self across various discrete behavioral states.Citation17–Citation23 (See also the literature referred to in the next paragraph.) Identity alterations observed in DID may also be considered as an elaborated version of trauma-related mental intrusions and avoidance that corresponds to the basic mechanism of post-traumatic stress disorder (PTSD).Citation24–Citation26 While the dynamics are similar, DID has discrete identities with their own first-person perspective (multiple “I” selves) and breaks in consciousness between these identities, which do not occur in PTSD.Citation4
More severe and earlier-onset child abuse appears to differentiate DID from other disorders.Citation27,Citation28 Large-scale clinical and epidemiological studies in the United States, Australia, Turkey, Puerto Rico, the Netherlands, Germany, and Canada have consistently found that DID is linked to antecedent chronic abusive experiences in childhood, typically at the hands of an attachment figure.Citation29–Citation31 A large representative sample of women from the general population in Turkey (N=994) was evaluated in three stages: after completing a self-report measure of dissociation, two groups of participants with high and low scores were administered the DDIS by a researcher blind to scores, followed by blinded clinical examination. The researchers were able to identify four cases of DID, all of whom reported childhood abuse and/or neglect.Citation32
Dalenberg et alCitation20 calculated Ross and Ness’Citation33 comparison of physical and sexual abuse in DID patients and controls, finding effect sizes of 0.74–0.78. By using corroborating documentation from hospital, police, and child protection agencies or witnesses, several studies have confirmed histories of severe abuse in DID.Citation29,Citation34,Citation35 In most clinical series, childhood abuse and/or neglect is reported by 90–100% of the patients directly during the study examination.Citation36,Citation37 Dissociative amnesia for childhood events may prevent such reports by some of the patients.Citation38
Milder presentations of DID are sometimes associated with traumatization that is covert, such as enduring severely dysfunctional communication and relationship styles in family members, including subtle forms of emotional neglect. In a study conducted on a large group of college students, Şar et alCitation39 demonstrated that emotional neglect predicted a dissociative disorder (including DID) diagnosis. Krüger and FletcherCitation37 demonstrated that self-reported emotional neglect by biological parents or siblings in childhood was the strongest individual predictor of an adult diagnosis of a dissociative disorder (including DID) in psychiatric patients (out of all other combinations of abuse type and abuser-abused relational ties).
Some data and theory suggest that disorganized attachment style may also underpin the development of DID.Citation40–Citation45 BowlbyCitation46 proposed that inadequate care-seeking interactions with primary caregivers could lead the infant to develop multiple internal representations of self and attachment figures (which he called internal working models [IWM]). Main and HesseCitation47 identified disorganized attachment developing from a relational context where the child who is seeking safety and comfort is frightened by the caregiver whom the child is pursuing for soothing or the child frightens the caregiver, thereby impeding connection. Contradictory IWM develop to represent the caregiver as dangerous and safe at the same time. These models activate in contexts of abuse to motivate protection from the same caregiver to whom safety seeking is also sought. Early-onset abuse and/or neglect by a relational figure is associated with disorganized attachment (and disorganized attachment may heighten the likelihood of abuse experiences). Hence, disorganized attachment may provide a foundation for DID.Citation40,Citation48
DID patients often feel very isolated/lonely, in the sense that they believe they are the only one in the universe who is “different” from others and that they do not understand themselves. Hence, they experience depersonalization and derealization that may go back to their childhood.Citation49 DePrince et alCitation50 found that alienation was the only cognitive appraisal variable to differentiate DID from PTSD. While the groups had similar appraisals of shame, betrayal, self-blame, anger, and fear, the DID participants had higher appraisal of themselves as experiencing alienation. This construct is associated with feeling alone, disconnected, and different.
Abuse and neglect may activate feelings of alienation, isolation, and loneliness, and such experiences may compound the impact of trauma and the development and maintenance of DID. If the necessary relational support to enable constructive processing of specific abuses is absent, the child is impeded in their ability to make sense of these experiences through narrative and the containment of the affective states activated, thus inhibiting the integration of the abuse with other autobiographical experiences. Consequently, the representations of abuse/neglect experiences remain isolated from integration, and with further incidences and isolation, the child’s ability to develop an ordinary sense of self-in-relation-to-others, based on a coherent narrative that includes the abuse experiences, is impeded and dissociative identities may begin to form. Interpersonal and internal phobias (e.g., phobias of other dissociative identities) then interfere with cooperation toward change, integration, and growth.Citation51,Citation52
High hypnotizability – itself a non-pathological, genetically derived capacity – has also been proposed to be a necessary diathesis for DID.Citation53 Although patients with DID have higher hypnotizability than those with other mental disorders, higher hypnotizability is also found in patients with chronic refractory post-traumatic states in general.Citation54–Citation56 Hence, data are required to determine the degree it represents a diathesis for DID that may reflect part of the biological contribution to the development of the disorder in the presence of other necessary factors.
Family, society, and culture DID can be found in all cultural settings.Citation57 Cultural processes influence the development and phenomenology of DID.Citation58,Citation59 The role of culture may be divided into two components: as the origin of trauma and as modifier of expression of the disorder. Although childhood abuse and neglect require the presence and actions of “perpetrators”, they can occur only in a suitable environment. This environment is characterized by denial, boundary violations, reality distortions, paranoia, narcissism, and dramatic posturing, which usually serves the purpose of maintaining the family structure. These features and dynamics may derive from psychological, relational, and economic needs of one or both of the parents, as well as oppressive traditions that do not allow a dissolution of marriage and other contextual issues in the family.Citation60
Dysfunctions in the family may partly originate from parents’ own traumatic antecedents that lead to inter-generational transmission of developmental stress as reported in the context of the “apparently normal (dissociative) family” by Öztürk and Şar.Citation61 In their empirical study, family members of patients with DID and related dissociative disorders reported frequent mood swings, intense anger and inability to control anger, transient dissociative experiences or paranoid ideas, and identity confusion more frequently than controls. Some of these features were correlated with certain types of childhood trauma in this group. For example, frequent mood swings were associated with all types of childhood trauma except sexual abuse, and identity confusion was correlated with emotional abuse.Citation61
In such a family with subclinical dissociative characteristics, individuals can interchange their social roles over time, alternating between being a victim, abuser, and rescuer.Citation62 Depending on their own traumatic past, or on their current interaction between each other and with their children, the parents may maintain trust and present themselves in a positive role (“angelic”, affectionate/compassionate parent), but they can turn to an abusive parenting style (angry, aggressive, insistent) at any time. The changing attitudes of their parents and the marital discord will often cause contradictory feelings within the children. Family members often feel trapped, first being unable to leave in the midst of a crisis as it is not safe. Then, they do not leave the family when the crisis is over and the need to escape has vanished, as the atmosphere becomes less threatening and more settled. Third, in an environment of neglect, chaos may be an opportunity for making contact with others in the unit.Citation61 Upon direct traumatization early in life, the ever-changing roles in an enduring family system continue to push children and adolescents to utilize a dissociative adaptation style in a period sensitive to the establishment of a stable identity.
Betrayal traumaCitation63 (i.e., trauma perpetrated by someone the victim relies on, e.g., by a primary caregiver)Citation64 is common in such family systems that are characterized by secrets and denial. Betrayal trauma theory suggests that dissociative amnesia is an adaptive response to childhood abuse that allows for survival by enabling the child to maintain attachment to an abusive figure who is also vital to his or her development. A recent study by Kaehler and FreydCitation65 found that higher betrayal traumas are associated with greater “borderline” characteristics that are common in DID as secondary features that do not necessarily point to an underlying personality disorder.Citation24,Citation38,Citation39,Citation49
As a possible example of the influence of culture as a modifier of the expression of DID, in a comparison of Turkish and Dutch patients with DID, large differences existed between the two groups in meeting borderline personality disorder criteria.Citation27,Citation36 Namely, Turkish patients reported intense anger and lack of control of this emotion, chronic feelings of emptiness and boredom, efforts to avoid abandonment, and intense but unstable relationships more frequently than Dutch patients. In turn, Dutch patients reported frequent mood swings, physically self-damaging acts, identity confusion, and impulsive and unpredictable behavior more frequently than Turkish patients. While such differences seem to originate from cultural factors, some types of affect dysregulation, possibly independent of cultural environment, were common to both groups. In another study – possibly as an indicator of the relational nature of the local culture – Turkish adolescent outpatients with dissociative disorders (including DID) differed from non-dissociative psychiatric outpatients on heightened prevalence of concurrent separation anxiety disorder.Citation4
Families constitute a subsystem in the broader context of society and culture. As presented in a South African example of culture as modifier of the expression of DID,Citation66 dissociation may help individuals or communities to survive in a world of conflicting messages, where conflict is often interpersonal/cultural/societal in nature, rather than primarily intrapsychic. The resultant fluctuating self-states – that might have been diagnosed as the dissociative identities of DID in a different cultural context – may be tolerated as normal expressions of societal conflict in a culture where conflicting ideologies pervade everyday life and where a normal sense of self is deeply dependent on a certain level of connectedness with others. Covering a subtler version of such systemic influence as well, Şar and ÖztürkCitation67 proposed a model of sociocognitive adaptation to developmental traumatization at the cost of internal detachment of the individual (“functional dissociation of the self ”).
The so-called sociocognitive model of DID (e.g., Lynn et alCitation68) went beyond recognizing the influence of sociocognitive factors on the development and phenomenology of DID. This model suggested that media reports, a high level of social knowledge about DID, influential and suggestive therapists, as well as patients’ own suggestibility, cognitive distortions and fantasy proneness all led patients to believe (wrongly) that they had dissociative identities. This view of DID markedly contrasts with the post-traumatic model of DID (outlined earlier), which proposes that dissociative identities are the primary results of early trauma and the relational, cognitive, emotional, and neurobiological consequences of it (along with other related factors as outlined in this paper) rather than primarily the result of social and cognitive forces. Moreover, the presence of sociocognitive forces does not provide any proof for iatrogenesis. Yet, sociocognitive and trauma models are not entirely contradictory,Citation69 as the trauma model, e.g., argues that social and cultural factors influence the presentation, but not typically the creation, of dissociative identities.Citation20,Citation69–Citation71 In fact, societal conditions themselves may also be the source of traumatic antecedents as observed in oppressive communities and traditions.Citation72
Cognitive etiological models and factors Memory and the construction of self-identity are cognitive processes that appear markedly and centrally disrupted in DID, such that the discriminating symptoms of the disorder are the experience of amnesia for autobiographical events and the presence (or experience) of non-integrated, dissociative identities. Consequently, cognitive processes are implicated in the etiology of DID. The way cognition is organized and the appraisals and beliefs associated with what autobiographical information is available for retrieval may give rise to dissociative identities and amnesia between them. The development of a sense of self is predicated on the collection of life experiences that are encoded as occurring to the self.Citation73 Thus, the construction of self is underpinned by episodic and semantic autobiographical memories laid down with autonoetic consciousness (i.e., this experience happened to me, and when I remember, it has the felt sense that I experienced it).Citation74 Memory an construction of seldf identity are cognitive processes that are negativeky imapcted by DID The way cognition is organized and the appraisals and beliefs associated with what autobiographical information is available for retrieval may give rise to dissociative identities and amnesia between them Thus, the construction of self is underpinned by episodic and semantic autobiographical memories laid down with autonoetic consciousness (i.e., this experience happened to me, and when I remember, it has the felt sense that I experienced it As such, an apparent etiological feature of dissociative identities is associated with the breakdown between encoding experienced events (i.e., the functioning of the human memory system) and perceiving ownership of those events as part of autobiographical experience (i.e., self-referencing the events). That is, there is a breakdown between memory and sense of self. Dissociative identities have their origin in memories of experienced events being owned or feeling like they relate to self in some identities but not others. Thus, different identities draw on, and feel ownership of, 1) different memories, 2) different aspects of the same experience, or 3) overlapping memories/experiences with different appraisals and narratives. Dissociative identities and the different bundles of owned memorized experience that characterize them may differ markedly from each other on lower order characteristics, such as physiological arousal (e.g., heart and respiration rate, blood pressure), affective tone, and neurobio-logical correlates (e.g., dominant brain activation), and higher order characteristics, such as the ability to have ownership of lived experiences, as well as appraise and narrate them.Citation14,Citation18,Citation75
Dissociative identities Kennedy et al have elucidated a cognitive perspective on the etiology of DID, drawing on the work of Beck.Citation76–Citation78 BeckCitation76 proposed that the personality is made up of “modes”, which contain cognitive, affective, behavioral, and physiological representations or schema for encoding experience and responding to internal and environmental demands. For example, a woman may have a “mother” mode that contains how she thinks, feels, behaves, and gets physiologically activated when caring for her child. These modes and the schema that make them up are mobilized by cues detected by what Beck called “orienting schema”, which appraise the internal and external landscape.
Cues identified by the orienting schema to indicate the requirements of child care will initiate, for instance, the mother mode. Under normal circumstances, this mode will be connected with other modes, such as the mode processing and responding to demands about the woman’s job or modes associated with defensive operations such as verbal aggression. All these modes are umbrellaed under the “conscious control system” that provides a means of unifying the multiple modes into a more integrated sense of self (i.e., a sense of “I” who has multiple ways of being and negotiating the world, via different modes or different “Me’s”). DID arises when modes become decoupled and exist in smaller, more isolated pockets (e.g., modes associated with relationship functioning, being a mother, and being a partner become decoupled from modes associated with occupational functioning).Citation77–Citation79
This decoupling creates multiple conscious control systems that capture the different and discontinuous arrays of modes, each having their own way of representing that aspect of self, based on the modes that make them up. The etiology of DID then, from a cognitive perspective, is related to the more enduring decoupling or dissociation of the association between modes and the development of different or unique first-person perspectives, or separate senses of self, based on the make-up of these non-coupled clusters of modes.
Amnesia Attempts to account for amnesia reported across different dissociative identities in clinical practiceCitation63,Citation76 initially drew on state-dependent memory phenomena as more controlled research began investigating memory anomalies across different identities. State-dependent memory refers to the superior recall of information encoded and retrieved in the same emotional state.Citation80 Alternatively, it is the process by which an individual fails to remember mundane information (e.g., where they left their phone) because they encoded the experience (putting their phone on the mantelpiece) in a different state of mind to that in which they are trying to retrieve the information. They may have encoded the information in a highly aroused state following a conflict with their partner and now in a calm state are attempting to find their phone.
Perhaps, the most elaborated framework of this theory for dissociative disorders is encompassed in Putnam’sCitation75 discrete behavioral states model. He argues that initially through biological decrees (need to feed, sleep) and then through experience (e.g., exposure to traumatic stress), different behavioral states come online and/or develop to support survival and promote adaptation to the environment.Citation18 These behavioral states differ not only in their manifest behavior (e.g., sleeping, feeding, socializing, escaping danger via fleeing) but also in all other psychophysiological dimensions, including arousal level, heart rate, motivation, affective tone, thought patterns and content, appraisals, and brain area activation.
PutnamCitation75 argues that trauma exposure leads to the development of discrete behavioral states that differ vastly in their psychophysiological make-up from other states of consciousness, giving rise to pathological dissociative symptoms and, in the most extreme case, dissociative identities. In the case of amnesia, it is proposed to be evident in situations where differences in state-dependent characteristics between encoding and retrieval are most distinct, so, e.g., retrieval failure when a state characterized by relatively minimal arousal is asked about an experience encoded in a high state of arousal (e.g., an episode of incestuous abuse).
In DID, amnesia across identities is accounted for by encoding in one identity that has a very different psychophysiological make-up than the identity attempting to retrieve the information. As a result, amnesia would be predicted to be more likely across identities that are vastly different in their biopsychosocial characteristics. This theory draws on mechanisms evident in normal cognitive functioning (i.e., state-dependent memory) to explain amnesia across dissociative identities. It is proposed to account for findings in research that suggested that information encoded in one dissociative identity may not be available in a dissociative identity reporting amnesia for that information.Citation81
Recent research examining amnesia across dissociative identities has required an elaboration of earlier theories in an attempt to address the etiology of amnesia in dissociative identities. This work has found, at least in patients presenting for treatment, that memories residing in another dissociative identity for which amnesia is perceived are actually available for retrieval or at least on objective assessment appear accessible.Citation82 This has prompted the question of whether amnesia across identities in DID is a cognitive process (i.e., associated with encoding characteristics and/or retrieval anomalies) or a metacognitive process (e.g., no encoding or retrieval deficits but a belief that content is not available). This latter explanation attempts to account for findings that representations of experience in memory appear to be accessible for retrieval in dissociative identities that believe they have no memory of such material.
Metacognitive processes, or more specifically metamemory processes, are involved in the monitoring, control, and appraisal of memories. They monitor for memories that fit goal-directed aims and assess them for subjective accuracy (e.g., the confidence in which the details retrieved feel accurate), they control which information is best to volunteer, and they subjectively appraise the ability to remember.Citation83
Huntjens et al draw on metacognitive processes to account for recent empirical findings, suggesting that amnesia in DID is not the result of being unable to access information but the result of believing that such information is inaccessible. She and her colleagues argued that, “[m]etamemory problems may lead patients not to acknowledge correctly retrieved material, which is believed to ‘belong’ to other identities, or indeed choose an incorrect answer alternative following the belief that the correct answer alternative cannot be known if the material that one is tested for was learned [or experienced] by another identity”.Citation84 The etiology of interidentity amnesia from this perspective is a metamemory belief that the material is unavailable rather than it being unavailable.Citation85 It resides in metamemory processes rather than in deficit memory functions. Consequently, the etiology of dissociative amnesia across identities may lie in information being encoded in a state (i.e., identity) that the retrieving identity, 1) believes they have no access to, and therefore gives up the search for such information, despite its availability, 2) appraises retrieval success as minimal, or 3) monitors with no confidence that retrieved information belongs to the self and therefore discards it.
While it remains to be examined empirically, the reported experience of amnesia across identities in DID may have its origin in retrieval states (i.e., dissociative identities) being psychobiologically distinct from encoding states (i.e., different dissociative identities). Such state-dependent processes may disrupt the search for and appraisal of encoded information (i.e., metamemory processes).
Neurobiology of DID Studies on the neurobiology of DID are in their infancy. They have focused mainly on two issues: differences between dissociative identities within patients with DIDCitation86 and differences between patients with DID and controls (the controls being either healthy subjects or other psychiatric patients). There are both structural and functional neuroimaging findings that demonstrate differences between dissociative patients and non-clinical populations. However, the specificity of these findings for DID would hinge on future comparisons with patients with other psychiatric disorders and whether the structural anomalies, e.g., are a cause or consequence of DID.
In positron emission tomography (PET) studies, when compared to a dissociative identity focused on the tasks of daily living, a dissociative identity focused on trauma memories and defensive operations showed increased cerebral blood flow in the amygdala, insular cortex, somatosensory areas in the parietal cortex, and the basal ganglia, as well as in the occipital and frontal regions and anterior cingulate.Citation87,Citation88 In a subsequent PET study, healthy controls simulating distinct dissociative identities were unable to reproduce the same network patterns as the DID patients.Citation86
In the quantitative electro-encephalogram (QEEG) study by Lapointe et al,Citation89 variability between identity states involved mostly beta activity in the frontal and temporal lobes. Hopper et alCitation90 demonstrated that the average alpha coherence on QEEG was lower for “alter” identities than for “host” identities (i.e., the identity predominantly engaging with the external world) in five DID patients in some temporal, frontal, parietal, and central regions.
In an functional magnetic resonance imaging (fMRI) study, women with DID and matched healthy female actors were compared in their responses (assessed both in “host” and ”emotionally laden” dissociative identities) when consecutively exposed to masked neutral and angry faces.Citation91 Differences between “host” and “emotionally laden” identities in DID patients and between DID and simulating controls were generally larger for neutral than angry faces. In DID, compared to “host”, “emotionally laden” dissociative identities were associated with more activation of the parahippocampal gyrus. Following neutral faces and compared to the “emotionally laden” identity in controls, “emotionally laden” identity in DID had more activation in brainstem, face-sensitive regions, and motor-related areas. There were neither significant within-group differences nor significant between-group differences in state anxiety. Controls were not able to simulate genuine “host” and “emotionally laden” dissociative identities.
A structural MRI study established that DID patients have smaller hippocampi and amygdalae than normal controls.Citation92 Ehling et alCitation93 also found reduced volumes in the parahippocampal gyrus of individuals with DID and strong correlations between reduction of parahippocampal volume and both cognitive-emotional and sensorimotor dissociation, in comparison with normal controls. In two single photon emission computerized tomography (SPECT) studies, DID patients exhibited orbitofrontal hypoperfusion in comparison with normal controls conducted in “host” identities.Citation94,Citation95 Bilaterally increased perfusion in prefrontal regions and occipital areas accompanied this in one of these studies.Citation95 In the other one, the “host” identity showed increased perfusion in the left (dominant hemisphere) lateral temporal region compared to healthy controls.Citation94 This lateralization was not replicated in a follow-up study.Citation95
Notwithstanding the possible effect of psychiatric comorbidity as a confounding factor (hence, it cannot be considered as specific to DID), the findings concerning orbitofrontal hypoperfusion do not seem to be at odds with the theoretical understanding of developmental neurobiology. Longitudinal neuroimaging studies suggest that the orbitofrontal cortex is one of the last regions in the brain to fully develop in humans.Citation95 A tensor-based morphometry investigation indicates that orbitofrontal cortex volumes are smaller in children who have suffered early aberrant parental care in the form of physical abuse and that these volumetric alterations are associated with difficulties children experience in various aspects of their social lives.Citation96 The orbitofrontal cortex is a key component of a circuit that aids in adaptation to changing environmental contingencies and plays an important role in the control of emotion and motivational states. In this regard, SchoreCitation97 reported that there is a relationship between the development of the orbitofrontal cortex, emotion regulation, and attachment. In accordance with these observations and based on a neurodevelopmental approach, ForrestCitation98 proposed an “orbitofrontal model” for DID, which integrates and elaborates on theory and research from four domains: the neurobiology of the orbitofrontal cortex and its protective inhibitory role in the temporal organization of behavior, the development of emotion regulation, the development of the self, and experience-dependent maturation of the orbitofrontal cortex. This model hypothesizes that the orbitofrontal cortex plays a critical role in the development of distinct mental states (i.e., dissociative identities) due to its inhibitory functions.
Conclusion and directions for future research Understanding the etiology of DID requires integration of trauma exposure, coping, cognitive, neurobiological, systemic, and developmental factors. These include traumatic experiences, family dynamics, child development, and attachment.Citation17,Citation63,Citation99 DID develops when a child is exposed to chaos, coercion, and overt severe physical and/or sexual abuse or, alternatively, to “apparently normal” dissociative families often with subtle neglect, disorganized attachment to caregivers, and misattuned communication styles.Citation59 While the role of the child’s biological capacity to dissociate to an extreme level is unclear yet, there is evidence demonstrating the neurobiological impact of developmental stress. The latter converges around an impairment of connectivity in the central nervous system in affected individuals. From a psychological point of view, multiple self-states that do not become integrated over time allow the child to compart-mentalize trauma-related cognitions and overwhelming and conflicting feelings of betrayal, terror, love, and shame.Citation13,Citation17 Overwhelmed by intense conflicting needs and emotions, the child is unable to integrate discrete behavioral and emotional states into a coherent or relatively integrated self according to the appropriate sociocultural construction of self.Citation17,Citation100 Further research on the etiology of DID should be able to link clinical and empirical dimensions while considering the four domains addressed in this paper: i.e., developmental traumatization, family and sociocultural factors, cognitive functioning, and neurobiological anomalies.
(8) Twenty-nine subjects participated in the brain imaging study: 11 patients with dissociative identity disorder (DID), 10 high fantasy prone DID simulating controls, and 8 low fantasy prone DID simulating controls. The controls were instructed to enact the two DID identity states: a neutral identity state (NIS) and a trauma-related identity state (TIS). Brain imaging data, autonomic (systolic and diastolic blood pressure, discrete heart rate and heart rate variability (HRV)) and subjective (controls’ subjective sensorimotor and emotional experiences) reactions were obtained. DID patients, as well as high fantasy prone and low fantasy prone controls were studied in the two different types of identity states during a memory script (MS) driven (neutral or trauma-related autobiographical texts) imagery paradigm. The brain imaging data of the three groups was statistically analyzed in SPM5 in a three-by-two-by-two factorial design which allows for the assessment of various effects, e.g., main effects and simple subtraction analyses (within and between identity state) within and between the three groups.
Abstract Background Dissociative identity disorder (DID) is a disputed psychiatric disorder. Research findings and clinical observations suggest that DID involves an authentic mental disorder related to factors such as traumatization and disrupted attachment. A competing view indicates that DID is due to fantasy proneness, suggestibility, suggestion, and role-playing. Here we examine whether dissociative identity state-dependent psychobiological features in DID can be induced in high or low fantasy prone individuals by instructed and motivated role-playing, and suggestion.
Methodology/Principal Findings DID patients, high fantasy prone and low fantasy prone controls were studied in two different types of identity states (neutral and trauma-related) in an autobiographical memory script-driven (neutral or trauma-related) imagery paradigm. The controls were instructed to enact the two DID identity states. Twenty-nine subjects participated in the study: 11 patients with DID, 10 high fantasy prone DID simulating controls, and 8 low fantasy prone DID simulating controls. Autonomic and subjective reactions were obtained. Differences in psychophysiological and neural activation patterns were found between the DID patients and both high and low fantasy prone controls. That is, the identity states in DID were not convincingly enacted by DID simulating controls. Thus, important differences regarding regional cerebral bloodflow and psychophysiological responses for different types of identity states in patients with DID were upheld after controlling for DID simulation.
Conclusions/Significance The findings are at odds with the idea that differences among different types of dissociative identity states in DID can be explained by high fantasy proneness, motivated role-enactment, and suggestion. They indicate that DID does not have a sociocultural (e.g., iatrogenic) origin.
Figures Figure 6Table 1Figure 1Table 2Figure 2Table 3Figure 3Figure 4Table 4Figure 5Figure 6Table 1Figure 1Table 2 Citation: Simone Reinders AAT, Willemsen ATM, Vos HPJ, den Boer JA, Nijenhuis ERS (2012) Fact or Factitious? A Psychobiological Study of Authentic and Simulated Dissociative Identity States. PLoS ONE 7(6): e39279. https://doi.org/10.1371/journal.pone.0039279
Editor: Jerson Laks, Federal University of Rio de Janeiro, Brazil
Received: March 5, 2012; Accepted: May 16, 2012; Published: June 29, 2012
Copyright: © 2012 Reinders et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: AATSR is supported by the Netherlands Organization for Scientific Research (www.nwo.nl), NWO-VENI grant no. 451-07-009. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Introduction Despite its inclusion in the Diagnostic Manual for Mental Disorders [1], the genuineness of dissociative identity disorder (DID) continues to be disputed. Supporters of the diametrically opposed trauma-related and non-trauma-related views have been engaged since decades in a passionate debate regarding its validity as a mental disorder, and whether it is related to traumatization or to fantasy proneness, suggestibility, suggestion, and simulation [2]–[10].
The non-trauma-related position [2], [3], [7], [11]–[13], also referred to as the sociocognitive model of DID [14]–[16], holds that DID is a simulation caused by high suggestibility and/or fantasy proneness [17]–[21], suggestive psychotherapy and other suggestive sociocultural influences (e.g., the media and/or the church). According to this model, “[t]he rules for enacting the [DID] role […] are as follows: (a) Behave as if you are two (or more) separate people who inhabit the same body. (b) Act as if the you I have been addressing thus far is one of those people and as if the you I have been talking to is unaware of the other coinhabitants. (c) When I provide a signal for contacting another coinhabitant, act as though you are another person. To the extent that patients behave in terms of these rules, the “classic” symptoms [of DID] follow by implication and do not have to be taught through direct instruction or further suggestion”, Spanos (p.239 [15]). Fantasy proneness and suggestibility are highly correlated [18], [22]–[25], and dissociative symptoms were found to be correlated with fantasy proneness, heightened suggestibility, and susceptibility to pseudomemories [11], [26].
To date, the position that DID is caused by sociocultural factors and personal features such as fantasy proneness has not been tested in studies involving DID patients, and evidence that the complex phenomenology and psychobiology of DID can be created and sustained over time by these factors is lacking [27]–[30]. Despite this lack of empirical support, the sociocognitive and fantasy based model of DID is influential in contemporary psychiatry and there have been proposals to prevent the inclusion of DID in the DSM-V [31].
The trauma-related perspective entails that DID is related to a combination of factors that include chronic emotional neglect and emotional, physical, and/or sexual abuse from early childhood, insufficient integrative capacity, attachment disorder, and lack of affect-regulation by caretakers [27], [32]–[35]. In this view DID is thought to be at the far end of the spectrum of trauma-related psychiatric disorders, i.e. being a severe form of post-traumatic stress disorder (PTSD) [33], [36].
Holders of the trauma-related view acknowledge that: some features of dissociative identity states can be influenced by sociocultural factors [33], that false positive cases of DID have evolved in a treatment setting, and that some psychiatric patients imitate DID [37]. However, they also note that there are differences between authentic and imitated DID and that there is no evidence that DID can (sub-)consciously be created by sociocultural factors [27]. Furthermore, even if DID symptoms can be created iatrogenically or enacted [14] this does not mean that genuine trauma-related DID does not exist [38].
According to the DSM-IV [1], DID is characterized by, among others, the presence of two or more distinct `identities’ or `personality states’. Different proposed labels include `different emotional states’, `alters’, `dissociative parts of the personality’ [33], and `dissociative identity states.’ Following previously used descriptions and terminology [39], [40] different types of dissociative identity states are indicated here as neutral identity states (NIS) and trauma-related identity states (TIS). These indicators are derived from the terms ‘apparently normal part of the personality (ANP)’ and ‘emotional part of the personality (EP)’ respectively, which are used in the theory of structural dissociation [33], [41]. This theory defines dissociation as a division of personality into different types of subsystems, each with their own first-person perspective, that is, their own point of view as to who they are, what the world is like, and how they relate to that world [42]. As NIS DID patients concentrate on functioning in daily life, commonly try to hide their pathology, and have not sufficiently integrated (e.g., have partial or complete amnesia) traumatic memories. That is, NIS fails to relate the trauma-related nature to its self [39]. In contrast, TIS does have conscious access to these memories, recalls them as personal experiences and is bodily and emotionally affected by them. That is, as TIS the patients are fixated in traumatic memories and engage in defensive actions such as freeze and flight, when they are or feel threatened [41], [43], thereby activating fast subcortical response routes in the brain [40], [44]. TIS who engage in active kinds of physical defence (e.g., freeze, flight, fight) would involve dominance of the sympathetic nervous system, whereas those who engage in total submission (i.e.,playing dead) would be primarily mediated by the dorsal vagal branch of the parasympathetic nervous system [45].
Proponents of the sociocognitive view have argued that the different patterns of subjective, psychophysiological, and neural activity for NIS and TIS in response to a trauma-memory script that Reinders et al. [39], [40] documented, might be due to fantasy proneness, suggestion and role-playing, and that they do not prove a traumagenic origin of DID. Obtaining independent proof of childhood traumatization in adulthood is most difficult. However, the claim that the previously reported results constitute effects of fantasy proneness, suggestion, and role-playing is open to test. Thus, the present study involves a psychobiological comparison between NIS and TIS engaging in active kinds of physical defence in DID patients (i.e., the DID identity states from Reinders et al. [39], [40]), and simulated NIS and TIS in high and low fantasy prone mentally healthy women who do not report a trauma history and who are instructed and motivated to role-play these different identity states (i.e., simulated identity states).
The a priori hypotheses of the current study were: (i) important previously found psychophysiological and neurobiological differences between NIS and TIS engaging in active kinds of physical defence in DID patients [39], [40] are upheld when controlling for fantasy proneness, suggestion, and instructed and motivated role-playing, and (ii) the upheld psychophysiological and neurobiological differences for NIS and TIS in DID patients include higher sympathetic nervous system activation (e.g. higher heart rate and systolic bloodpressure) and subcortical activity (e.g. the amygdala and caudate nucleus) for TIS in DID, and (iii) hyperactivation of the cortical multimodal posterior association areas (e.g. the intraparietal sulcus and (pre-)cuneus) for NIS in DID when listening to personal trauma scripts.
Results Twenty-nine subjects participated in the brain imaging study: 11 patients with dissociative identity disorder (DID), 10 high fantasy prone DID simulating controls, and 8 low fantasy prone DID simulating controls. The controls were instructed to enact the two DID identity states: a neutral identity state (NIS) and a trauma-related identity state (TIS). Brain imaging data, autonomic (systolic and diastolic blood pressure, discrete heart rate and heart rate variability (HRV)) and subjective (controls’ subjective sensorimotor and emotional experiences) reactions were obtained. DID patients, as well as high fantasy prone and low fantasy prone controls were studied in the two different types of identity states during a memory script (MS) driven (neutral or trauma-related autobiographical texts) imagery paradigm. The brain imaging data of the three groups was statistically analyzed in SPM5 in a three-by-two-by-two factorial design which allows for the assessment of various effects, e.g., main effects and simple subtraction analyses (within and between identity state) within and between the three groups.
Autonomic and Subjective Reactions Statistical results of the autonomic and subjective reactions analyses between the three groups are presented in Table 1. Mean values and the direction of the responses are depicted in Figure 1. Significant differences were found for most of the measured variables between the DID patients and both control groups (see for details Table 1) for dissociative identity state (DIS), DIS*group, MS, MS*group, DIS*MS, and DIS*MS*group.
Figure 1. Graphical representation of averages and direction of subjective emotional experiences, subjective sensori-motor experiences, and cardiovascular responses.
The dashed line depicts the response of the neutral identity state (NIS) when listening to the neutral or trauma-related memory script (MS). The solid line depicts the response of the traumatic identity state (TIS) when listening to the neutral or trauma related MS. All three groups are presented per variable: the dissociative identity disorder patients (DID) in pink, the high fantasy prone DID simulating controls (CH) in cyan and the low fantasy prone DID simulating controls (CL) in blue. See Table 1 for the statistical values.
Regional Cerebral Blood Flow Changes Covariate data. T-tests were used to test if a significant (p<0.05) difference in regional cerebral bloodflow (rCBF) variance between the DID and control groups was explained by the subjective or objective covariates (i.e. the principal components (PC), see below). No brain areas for which a significant difference was present between the DID patients and the high or low fantasy prone controls respectively were found.
Comparing Simulated and Pathological Identity States Main effects and conjunction analyses. Results for the within DID group re-analyses and for the two between group comparisons of the dissociative identity states (DIS) main effects, both TIS and NIS, are given in Table 2. Significant differences in rCBF changes between the DID and both the high and low fantasy prone groups were found, i.e., text independent effects. These findings are shown in Figure 2. Commonalities in brain activation between patients and controls were found (data not shown).
Trauma-related MS effects within identity state. Trauma-related MS effects within both TIS and NIS are given in Table 3. TIS showed significant regionally specific increases and decreases in cerebral blood flow, when processing the trauma-related MS as compared to the neutral MS, between the DID and both the high and low fantasy prone control groups. These findings are depicted in Figure 3 and 4.
Trauma-related MS effects between identity state. Trauma-related MS effects between DIS are given in Table 4. Different rCBF patterns were found for NIS and TIS, when processing the trauma-related MS, between the DID and both the high and low fantasy prone control groups. These differential rCBF patterns are shown in Figure 5 and 6. The results indicate that, for some areas (e.g. the parahippocampal gyrus in the comparison NISt-TISt or the caudate nucleus in the comparison TISt-NISt), the difference in blood flow between patients and controls is larger than the difference between the DID identity states. Figure 3. “Glass brain” renderings show differences in the processing of the trauma-related text (indicated with a small ‘t’) and the neutral text (indicated with a small ‘n’) within the trauma-related identity state (TIS).
Differences in regional cerebral blood flow patterns for the dissociative identity disorder (DID) group (left) and the comparison of this group to the high (middle) and low (right) fantasy prone DID simulating controls (CH and CL respectively) are depicted. See Table 3 for the specific areas.
the left amygdala, the left insula, the left precuneus, and the right occipitotemporal sulcus. These areas have the most significant rCBF differences between the dissociative identity disorder patients and high and low fantasy prone DID simulating controls (CH and CL respectively) and is shown both in directionality, i.e. the bar graphs, and location, i.e. shown on a coronal overlay (left in the picture is left in the brain). Results show the differential processing of the trauma-related text versus the neutral text within the TIS, when comparing the DID groups to the high fantasy prone control group (left) and low fantasy prone control group (right).
Discussion The present study was performed to examine whether earlier reported results [39], [40] for DID hold after correcting for potential iatrogenic and other sociogenic effects. To this end, we tested whether these findings can be simulated by motivated role-enactment and/or is facilitated by a high level of fantasy proneness [18] by re-investigating the patient population from Reinders et al. [39], [40]. Results of a sub-study (see Methods and Supporting Information S1) show that DID patients have a fantasy proneness score of 9.83 (SD 5.25), which approximates the normal population, indicating that fantasy proneness might not play a major role in DID. This finding is consistent with the current psychobiological results. Neither high nor low fantasy prone healthy controls, instructed and motivated to simulate two different types of dissociative identity states in DID (i.e., NIS and TIS), mimicked previously observed psychophysiological and neural reactions that are associated with these identity states in DID [39], [40], which is supportive of our first a priori hypothesis.
Differences in regional cerebral bloodflow patterns for the dissociative identity disorder (DID) group (left) and the comparison of this group to the high (middle) and low (right) fantasy prone DID simulating controls (CH and CL respectively) are depicted. See Table 4 for the specific areas.
Figure 6. The brain areas indicated with the blue cross (i.e. the peak voxel) are (from top left to bottom right): the right caudate nucleus (dorsal part) (2x), the left precuneus, and the right occipitotemporal sulcus.
These areas involve the most significant rCBF difference between the dissociative identity disorder patients and high and low fantasy prone DID simulating controls (CH and CL respectively) and is shown in both directionality, i.e. the bar graphs, and location, i.e. shown on a coronal overlay (left in the picture is left in the brain). Results show the differential processing of the trauma-related text between the TIS and the NIS, when comparing the DID groups to the high fantasy prone control group (left) and low fantasy prone control group (right).
From results shown in Figures 2, 3, and 5 a general feel of the effects can be obtained. Figures 2 and 5 and the top row of Figure 3 show that in the high fantasy prone control group more of the original DID rCBF patterns are apparent, while the low fantasy prone control group show less similarities with the original DID rCBF patterns, for example the disappearance of the left amygdala activation. Less similarities between patients only and patients versus controls means more overlap in rCBF patterns. In other words the less differences in the rCBF patterns between patients only and patients versus controls, the better the controls simulate DID. Thus, relatively speaking, low fantasy prone controls simulated the performance of DID patients better than high fantasy prone controls. This result is the opposite from the direction indicated by holders of the sociocognitive and fantasy based model of DID [17], [19]–[21], [46]. As patients and controls were scanned in a highly similar experimental setting and because controls were highly motivated to simulate DID, commonalities in brain activation between patients and controls were expected. Despite the overlap in brain activation between patients and controls important previously found psychophysiological and neurobiological differences between NIS and TIS in DID patients were upheld when controlling for fantasy proneness, suggestion, and instructed and motivated role-playing, which is supportive of our first a priori hypothesis.
The activated areas seem to be subdivided in two distinct neural networks, where the NIS activates areas in the cerebral cortex, while the TIS mainly activates subcortical areas (e.g., see Table 2 and Figure 2). The Tables show a detailed listing of all the brain areas involved. The brain areas marked with a II in the Tables are brain areas non-specific to DID as they disappear after comparing to a control group, i.e. these areas share commonalities between patients and controls. The brain areas marked with a III and IV in the Tables are brain areas specific to DID. The areas in the latter group are areas that were not reported earlier as they were “subtracted out” in the within group comparisons.
Our findings support the cortico-limbic inhibition model of trauma-related dissociative disorders [41], [47]. Results of both the NISt-TISt comparison and the main effect of NIS show significant overlap with the activated network of brain regions during emotional memory suppression of unwanted memories in mentally healthy individuals [48], for example in frontal areas (BA 4/6/8/10/47), cingulate cortex (BA 32), and intraparietal sulcus (BA 7/40). Anderson et al. [48] did not find all of these brain areas. There is significant overlap between our study and their study, but the brain areas involved in the modulation of access to trauma-related memory in our patient population are of larger number. This might be an indication that, when functioning as NIS, in DID patients different cortical processes are involved that modulate conscious and subconscious perception of trauma-related information. These areas, e.g. (pre-)cuneus (BA 7/39, 18/19), fusiform gyrus (BA 18/19/37), lingual gyrus (BA 18), occipital gyrus (BA 18/19/37), and the parahippocampal gyrus (BA 35/36), are located in the posterior association areas (PAA) and have been indicated to be involved in multimodal [49], [50] somato-sensory integration [51], [52] of information, especially in relation to attention and perceptual awareness [49]. Hyperactivation of cortical multimodal association areas for NIS in DID when listening to personal trauma scripts constituted our third a priori hypothesis. We thus propose that for emotional memory suppression, or NIS’ mental avoidance [41], of unwanted memories in DID the PAA fulfils a pivotal role.
There are notable similarities in the patterns of brain activation for DID patients, as revealed in the main effect TIS and the TISt-NISt comparison, and mentally healthy individuals unsuppressed memory retrieval [48]. Both groups had increased activation of the insula (BA 13) and parietal operculum (BA 40/43). We did not find the hippocampus to play a role in memory retrieval in DID patients, despite the fact that this area has been indicated in memory processing in mentally healthy individuals [48]. Instead we found that the caudate nucleus was activated when DID patients listened to the trauma-memory scripts as TIS. Acute stress can be associated with a shift from hippocampal involvement to caudate nucleus involvement [53], [54]. Thus, acute stress is linked with caudate nucleus-dependent stimulus-response type reactivity at the expense of hippocampal dependent spatial learning and memory [53]. According to the theory of structural dissociation [33], [41] listening to a description of a personal traumatic memory in an experimental setting constitutes a consciously experienced acute stressor for TIS, because as this dissociative identity state DID patients do not manage to mentally avoid the relevant memory. When DID patients as TIS are confronted with reminders of traumatic memories, they may initiate a caudate mediated reflex-like flight-fright-freeze response [55], [56] which reaction is also supported by an accompanying amygdala activation [44], [57]. Another, but compatible, explanation for increased caudate and amygdala activation in DID patients as compared to controls is a heightened memory sensitivity for negative valanced information [58]. These findings for TIS are supportive of our second a priori hypothesis.
To date, experimental research of inter-identity amnesia in DID has produced mixed results. One study [59] demonstrated evidence for inter-identity amnesia, which is in line with the current findings. Other studies [60]–[65] found inter-identity transfer of newly learned non-autobiographical stimuli, even though the “amnestic” identity reported subjective amnesia for these stimuli. Several principles might explain the inconsistent findings: (i) Inter-identity amnesia may only exist for stimuli that have personal relevance for the “amnestic” identity. In the cited studies [59]–[65], it was not assessed if or to what degree the applied stimuli had autobiographical meaning for the tested “amnestic” and “mnestic” dissociative identities. Our study included traumatic memories that were subjectively autobiographical for TIS but not for NIS, and found that NIS and TIS had different subjective, psychophysiological, and neural reactions to a description of the involved traumatic memories. We also found that as a NIS, DID patients did not relate these traumatic memories to themselves [39]. These results indicate the importance of using autobiographical information when investigating inter-identity amnesia in DID. (ii) Inter-identity amnesia may predominantly exist between different types of dissociative identities, particularly between neural and trauma-related identity states.This has been clinically observed, theoretically proposed [33], [41] and is in line with our results. Unfortunately, in most studies [59]–[66] it was not assessed what types of dissociative identities participated, e.g. NIS or TIS. Therefore, we strongly recommend that in future research in DID the types of dissociative identities are verified and reported and that test material is used that is subjectively autobiographical for one dissociative identity, but not for another.
The sociocognitive view of DID entails the idea that this disorder can be easily and readily created in motivated suggestible individuals and that few suggestions would suffice to generate the symptoms of DID [15] (see Supporting Information S2). Still, one might argue that the current brief practice of DID simulation is insufficient to simulate the psychobiological profiles of NIS and TIS. Even if years of practice could generate these profiles, our findings suggest that fantasy proneness is not the driving factor because low fantasy prone controls simulated the performance of DID patients better than high fantasy prone controls. This result is the opposite from the direction indicated by holders of the sociocognitive and fantasy based view. Therefore we feel that our study provides an important contribution to the etiology discussion.
For the first time, it is shown using brain imaging that neither high nor low fantasy prone healthy women, who enacted two different types of dissociative identity states, were able to substantially simulate these identity states in psychobiological terms. These results do not support the idea of a sociogenic origin for DID.
Methods Somatic dissociation
Phsycological affects/symptoms
Memory, function, safety, risk factors for other disorderrs, For this i think its important to speak with survivors
NSC transplantation therapy (8)
NSCs are a promising treatment modality for diseases associated with the nervous system as they secrete soluble factors and differentiate into neurons, astrocytes and oligodendrocytes.
NSCs can be derived from three different sources using recent technical advances: direct isolation from primary tissues, differentiation from pluripotent stem cells and transdifferentiation from somatic cells.
Cell therapies based on NSC transplantation for the treatment of various neural defects and injuries in animal models and clinical trials have been widely investigated. The establishment of cell isolation and cell culture techniques has led to the development of favorable experimental methods and the identification of a rich cell source for NSC research. In 1992, Reynolds and Weiss isolated NSCs from the striatum of the adult mouse brain and reported the first use of epidermal growth factor (EGF) to induce NSC proliferation in vitro.1 Two years later, they found that the subependymal region in the mouse brain is the source of NSCs in vivo.2 Based on previous results, Weiss further reported that EGF and basic fibroblast growth factor (bFGF) cooperatively induce the proliferation, self-renewal and expansion of NSCs isolated from adult mouse thoracic spinal cord.3 NSCs can grow in single-cell suspensions obtained by enzymatic digestion and form spherical clusters called neurospheres, which are non-adherent and can be re-plated in selective culture medium to obtain neural cells.4, 5 Neurospheres can also be sub-cultured to expand the pool of NSCs for experimental or therapeutic purposes. Periventricular regions and olfactory bulb in adult mammalian brains are rich sources of NSCs.6, 7, 8 Beyond these methods of isolating NSCs through diverse culturing strategies, NSCs can also be directly isolated by cell sorting based on the expression of NSC surface markers.9 Belenguer and Guo have developed an optimized protocol for the isolation, culture and expansion of NSCs from mammalian animals.10, 11 Although, a canonical protocol for obtaining human tissue-derived NSCs has not yet been established, the technical methods are generally similar to the ones applied in animals, and the tissues must be obtained in accordance with ethical guidelines. Nervous system diseases are refractory diseases that can cause loss of sensation, loss of motor function and memory failure, as well as directly threaten the life of a patient. Currently, the pathogenic factors involved in these diseases and their pathogenesis are unclear. Traditional drug treatments are used to delay disease progression and cannot restore function or regenerate tissues. Recent studies have indicated that the transplantation of neural stem cells (NSCs) is a promising treatment modality for diseases associated with the nervous system, for the regeneration of neural cells and for the restoration of the microenvironment at the injury site (Figure 1). The cell source is the first issue that must be addressed to enable the application of NSCs in clinical treatments because the cell dose required for adequate transplantation is very high. NSCs can be derived from three different sources using recent technical advances, including direct extraction from primary tissues, differentiation from pluripotent stem cells and transdifferentiation from somatic cells (Figure 2 and Table 1).
NSC migration (9)
Migration toward pathology is the first critical step in stem cell engagement during regeneration. Neural stem cells (NSCs) migrate through the parenchyma along nonstereotypical routes in a precise directed manner across great distances to injury sites in the CNS, where they might engage niches harboring local transiently expressed reparative signals. The molecular mechanisms for NSC mobilization have not been identified. Because NSCs seem to home similarly to pathologic sites derived from disparate etiologies, we hypothesized that the inflammatory response itself, a characteristic common to all, guides the behavior of potentially reparative cells. As proof of concept, we show that human NSCs migrate in vivo (including from the contralateral hemisphere) toward an infarcted area (a representative CNS injury), where local astrocytes and endothelium up-regulate the inflammatory chemoattractant stromal cell-derived factor 1α (SDF-1α). NSCs express CXC chemokine receptor 4 (CXCR4), the cognate receptor for SDF-1α. Exposure of SDF-1α to quiescent NSCs enhances proliferation, promotes chain migration and transmigration, and activates intracellular molecular pathways mediating engagement. CXCR4 blockade abrogates their pathology-directed chain migration, a developmentally relevant mode of tangential migration that, if recapitulated, could explain homing along nonstereotypical paths. Our data implicate SDF-1α/CXCR4, representative of the inflammatory milieu characterizing many pathologies, as a pathway that activates NSC molecular programs during injury and suggest that inflammation may be viewed not simply as playing an adverse role but also as providing stimuli that recruit cells with a regenerative homeostasis-promoting capacity. CXCR4 expression within germinal zones suggests that NSC homing after injury and migration during development may invoke similar mechanisms.
BNDF increase
How do antidepressants elicit an antidepressant response? Here, we review accumulating evidence that the neurotrophin brain-derived neurotrophic factor (BDNF) serves as a transducer, acting as the link between the antidepressant drug and the neuroplastic changes that result in the improvement of the depressive symptoms. Over the last decade several studies have consistently highlighted BDNF as a key player in antidepressant action. An increase in hippocampal and cortical expression of BDNF mRNA parallels the antidepressant-like response of conventional antidepressants such as SSRIs. Subsequent studies showed that a single bilateral infusion of BDNF into the ventricles or directly into the hippocampus is sufficient to induce a relatively rapid and sustained antidepressant-like effect. Importantly, the antidepressant-like response to conventional antidepressants is attenuated in mice where the BDNF signaling has been disrupted by genetic manipulations. Low dose ketamine, which has been found to induce a rapid antidepressant effect in patients with treatment-resistant depression, is also dependent on increased BDNF signaling. Ketamine transiently increases BDNF translation in hippocampus, leading to enhanced synaptic plasticity and synaptic strength. Ketamine has been shown to increase BDNF translation by blocking NMDA receptor activity at rest, thereby inhibiting calcium influx and subsequently halting eukaryotic elongation factor 2 (eEF2) kinase leading to a desuppression of protein translation, including BDNF translation. The antidepressant-like response of ketamine is abolished in BDNF and TrkB conditional knockout mice, eEF2 kinase knockout mice, in mice carrying the BDNF met/met allele, and by intra-cortical infusions of BDNF-neutralizing antibodies. In summary, current data suggests that conventional antidepressants and ketamine mediate their antidepressant-like effects by increasing BDNF in forebrain regions, in particular the hippocampus, making BDNF an essential determinant of antidepressant efficacy.
Overall neurotrpohin increase
A number of studies have demonstrated that both morphological and biochemical indices in the brain undergo alterations in response to environmental influences. In previous work we have shown that rats raised in an enriched environmental condition (EC) perform better on a spatial memory task than rats raised in isolated conditions (IC). We have also found that EC rats have a higher density of immunoreactivity than IC rats for both low and high affinity nerve growth factor (NGF) receptors in the basal forebrain. In order to determine if these alterations were coupled with altered levels of neurotrophins in other brain regions as well, we measured neurotrophin levels in rats that were raised in EC or IC conditions. Rats were placed in the different environments at 2 months of age and 12 months later brain regions were dissected and analyzed for NGF, brain-derived neurotrophic factor (BDNF), and neurotrophin-3 (NT-3) levels using Promega ELISA kits. We found that NGF and BDNF levels were increased in the cerebral cortex, hippocampal formation, basal forebrain, and hindbrain in EC animals compared to age-matched IC animals. NT-3 was found to be increased in the basal forebrain and cerebral cortex of EC animals as well. These findings demonstrate significant alterations in NGF, BDNF, and NT-3 protein levels in several brain regions as a result of an enriched versus an isolated environment and thus provide a possible biochemical basis for behavioral and morphological alterations that have been found to occur with a shifting environmental stimulus.
TDP-43 reduction
Background TAR DNA-binding protein 43 (TDP-43) is a protein that is involved in the pathology of Amyotrophic Lateral Sclerosis (ALS) and Frontotemporal Lobar Degeneration (FTLD). In patients with these neurodegenerative diseases, TDP-43 does not remain in its normal nuclear location, but instead forms insoluble aggregates in both the nucleus and cytoplasm of affected neurons.
Results We used high density peptide array analysis to identify regions in TDP-43 that are bound by TDP-43 itself and designed candidate peptides that might be able to reduce TDP-43 aggregation. We found that two of the synthetic peptides identified with this approach could effectively inhibit the formation of TDP-43 protein aggregates in a concentration-dependent manner in HeLa cells in which a mutated human TDP-43 gene was overexpressed. However, despite reducing aggregation, these peptides did not reduce or prevent cell death. Similar results were observed in HeLa cells treated with arsenite. Again we found reduced aggregation, in this case of wild type TDP-43, but no difference in cell death.
Conclusions Our results suggest that TDP-43 aggregation is associated with the cell death process rather than being a direct cause.
Need brain scans of
- Healthy controls
- DID
- Bipolar disorder
- Schizophrenia
- Borderline personality disorder
- Ptsd
- C Ptsd
- depression
Common misdiagnoses
All from Other Disorders. (Jan 12, 2026). Traumadissociation.com. Retrieved Jan 12, 2026 from https://traumadissociation.com/other. Read more: https://traumadissociation.com/other (copy and pasted)
Bipolar Disorder
involves changes in mood that cycle between Depression and either mania (or the less severe hypomania), and sometimes "mixed episodes" which have features of both. In Dissociative Identity Disorder there are also frequent mood changes, these rapidly switching moods (within minutes or hours) are commonly caused by the presence of alters which have different moods, and the changes in moods can be puzzling to the person. The common misdiagnosis is Bipolar Disorder type 2, which involves hypomania rather than full mania, however mood changes in Bipolar Disorder do not switch back and forth as rapidly as those in Dissociative Identity Disorder.[2]:296
Schizophrenia
includes a range of different possible symptoms and is a Psychotic Disorder, and a spectrum of Schizophrenia symptom disorders exist. All the Schizophrenia symptom disorders involve a break with reality. [2] In Dissociative Identity Disorder reality testing is described as being "in tact". Hearing voices, which are actually the communication of alter personalities is very common in DID, hearing voices may also present in Schizophrenia but in a slightly different way, and many of the symptoms historically used to diagnose symptoms of Schizophrenia are more common in Dissociative Identity Disorder - these are known as Schneiderian first-rank symptoms (FRS). See passive influence in Dissociative Identity Disorder for a description of these symptoms. Amnesia is a required symptom of DID but not a diagnostic symptom in Schizophrenia.[2]
Borderline Personality Disorder
has many symptoms that overlap with the self-destructive behaviors common in Dissociative Identity Disorder, as well as symptoms that overlap with Complex PTSD (see below). The majority of people with Dissociative Identity Disorder also have Complex PTSD, and many have a diagnosis for Borderline Personality Disorder too (although these symptoms in DID may effect just the "host" identity or just specific alters).
Posttraumatic Stress Disorder
is very common in people with Dissociative Identity Disorder, both should be diagnosed if both are present. Symptoms that may occur in both DID and PTSD are: amnesia for some aspects of trauma, flashbacks (i.e., a sense of disconnection from the present while reliving the trauma - for instance less awareness of the person's surroundings), and lastly the combination of post-traumatic symptoms of intrusion and avoidance, negative alterations in cognition and mood, and hyperarousal that are part of PTSD's diagnostic criteria. Symptoms of Dissociative Identity Disorder that are not found in PTSD are: 1) amnesias for many everyday (i.e., nontraumatic) events, which is greater than ordinary forgetfulness 2) flashbacks which are followed by amnesia for the traumatic content of the flashback 3) disruptive intrusions (unrelated to traumatic material) by alter identities into the individual's sense of self and agency, and 4) infrequent, full-blown changes (switches) between alters. [3]:296
Complex PTSD (C-PTSD)
is commonly comorbid with Dissociative Identity Disorder. [5]:135 Complex PTSD is a well-recognized condition which involves additional symptoms beyond those needed for a PTSD diagnosis. Differences between Complex PTSD and Dissociative Identity Disorder are the described in the PTSD section above. Complex PTSD is not a DSM diagnosis (only PTSD and its dissociative subtype are) but many of Complex PTSD's symptoms and wider effects are listed in both the DSM-5's Additional Features Supporting Diagnosis and the Risk and Prognostic Factors sections for DID, and in the DID/DDNOS or Complex PTSD treatment guidelines. Dissociative Identity Disorder and Complex PTSD have many similarities, and certain symptoms or factors are common in both: self-injury/self-mutilation, in DID this is more common in women/girls than in men/boys frequent suicidal behavior/suicidality, 70% of people with DID have attempted suicide dissociative flashbacks alterations in attention and consciousness (e.g. dissociation) - a core symptom in both conditions child abuse is a known cause of both Complex PTSD and DID, but not the only possible cause many comorbid disorders, especially depression, anxiety and substance abuse (drug abuse) borderline personality disorder co-occurs in around 33% of people with Complex PTSD and 30-70% of people with DID risk-taking or high-risk behavior interpersonal relationship problems may be a Functional Consequence of DID feelings of shame, which may involve underreporting symptoms (especially in DID) revictimization: experiencing violent or abusive relationships, including in adulthood somatization - physical illness or problems which are medically unexplained - a core symptom in Complex PTSD
Unexplained neurological symptoms
are particularly common in DID, including non-epileptic seizures, Conversion Disorders (e.g., paralysis or sensory loss), and Somatic Symptom Disorders. The Somatoform Dissociation Questionnaire screening tool can help a clinician diagnose whether DID or OSDD is present. body image distortions In DID this may be linked to different identities: "Individuals may report that their bodies feel different (e.g., like a small child, like the opposite gender, huge and muscular). Alterations in sense of self and loss of personal agency may be accompanied by a feeling that these attitudes, emotions, and behaviors—even one's body—are 'not mine' and/or are 'not under my control'." [2]:293 the core PTSD symptoms (required in Complex PTSD): avoiding trauma reminders, re-experiencing trauma, negative thoughts/mood linked to trauma, problems with hyperarousal (e.g., being irritable or jumpy, sleep problems); most people with DID develop PTSD. [2]:280, 294-295, 297-298, [4], [5]:24, 127, 135-136, [7]:4, 11 Read more: https://traumadissociation.com/other
Accompanying disorders
- anywhere between 80 and 100% of individuals with DID who receive treatment also have symptoms of posttraumatic stress disorder (PTSD - see section on PTSD)
- Individuals with DID have very high rates of self-destructive and suicidal behavior and often have multiple, usually unproductive, hospitalizations for mood disorders, personality disorders, and/or psychotic diagnoses. The average individual with DID spends five to 12.5 years in mental health treatment until a correct diagnosis is made.
Experts in DID neuroanatomy
Blihar, D., Delgado, E., Buryak, M., Gonzalez, M., & Waechter, R. (2020). A systematic review of the neuroanatomy of dissociative identity disorder. European Journal of Trauma & Dissociation, 4(3), Article 100148. Lauren A.M. Lebois, McLean Hospital, Belmont, Massachusetts; Department of Psychiatry, Harvard Medical School, Boston, Massachusetts
David A. Ross, Department of Psychiatry, Yale University School of Medicine, New Haven, Connecticut
Milissa L. Kaufman, McLean Hospital, Belmont, Massachusetts; Department of Psychiatry, Harvard Medical School, Boston, Massachusetts
Smaller hippocampal volume has been reported in individuals with post-traumatic stress disorder (PTSD) and dissociative identity disorder (DID), but the regional specificity of hippocampal volume reductions and the association with severity of dissociative symptoms and/or childhood traumatization are still unclear. Brain structural magnetic resonance imaging scans were analyzed for 33 outpatients (17 with DID and 16 with PTSD only) and 28 healthy controls (HC), all matched for age, sex, and education. DID patients met criteria for PTSD (PTSD-DID). Hippocampal global and subfield volumes and shape measurements were extracted. We found that global hippocampal volume was significantly smaller in all 33 patients (left: 6.75%; right: 8.33%) compared with HC. PTSD-DID (left: 10.19%; right: 11.37%) and PTSD-only with a history of childhood traumatization (left: 7.11%; right: 7.31%) had significantly smaller global hippocampal volume relative to HC. PTSD-DID had abnormal shape and significantly smaller volume in the CA2-3, CA4-DG and (pre)subiculum compared with HC. In the patient groups, smaller global and subfield hippocampal volumes significantly correlated with higher severity of childhood traumatization and dissociative symptoms. These findings support a childhood trauma-related etiology for abnormal hippocampal morphology in both PTSD and DID and can further the understanding of neurobiological mechanisms involved in these disorders.
https://pubmed.ncbi.nlm.nih.gov/25545784/
https://www.ncbi.nlm.nih.gov/books/NBK553239/
Neuroanatomical evidence on the relationship between posttraumatic stress disorder (PTSD) and dissociative disorders is still lacking. We acquired brain structural magnetic resonance imaging (MRI) scans from 17 patients with dissociative identity disorder (DID) and co-morbid PTSD (DID-PTSD) and 16 patients with PTSD but without DID (PTSD-only), and 32 healthy controls (HC), and compared their whole-brain cortical and subcortical gray matter (GM) morphological measurements. Associations between GM measurements and severity of dissociative and depersonalization/derealization symptoms or lifetime traumatizing events were evaluated in the patient groups. DID-PTSD and PTSD-only patients, compared with HC, had similarly smaller cortical GM volumes of the whole brain and of frontal, temporal and insular cortices. DID-PTSD patients additionally showed smaller hippocampal and larger pallidum volumes relative to HC, and larger putamen and pallidum volumes relative to PTSD-only. Severity of lifetime traumatizing events and volume of the hippocampus were negatively correlated. Severity of dissociative and depersonalization/derealization symptoms correlated positively with volume of the putamen and pallidum, and negatively with volume of the inferior parietal cortex. Shared abnormal brain structures in DID-PTSD and PTSD-only, small hippocampal volume in DID-PTSD, more severe lifetime traumatizing events in DID-PTSD compared with PTSD-only, and negative correlations between lifetime traumatizing events and hippocampal volume suggest a trauma-related etiology for DID. Our results provide neurobiological evidence for the side-by-side nosological classification of PTSD and DID in the DSM-5. https://pubmed.ncbi.nlm.nih.gov/25670646/
https://medlineplus.gov/ency/article/002344.htm https://www.spinalcord.com/blog/gray-matter-vs-white-matter-in-the-brain
Background: Experiencing repeated childhood traumatisation impacts brain structure and function in individuals with dissociative identity disorder (DID) and post-traumatic stress disorder (PTSD). Quantitative grey matter neuroimaging research has shown aberrant volumes in traumatised individuals, however studies examining white matter are sparse, particularly for DID. The present study aims to examine white matter alterations of people with trauma-related disorders. Methods: Sixty-five female participants were included in this study: 33 diagnosed with a trauma-related disorder, namely 17 with DID and 16 with PTSD, and 32 healthy control (HC) participants. All participants underwent diffusion tensor imaging (DTI) and completed dissociation and traumatisation self-report measures. White matter integrity was characterised using voxel-based analysis (VBA), with network lesion mapping used to identify the implicated grey matter end points of the VBA findings.
Results: Between-group VBA comparisons showed reduced fractional anisotropy (FA) for participants with DID compared to HCs in bilateral pallidum (implicating striatal projections to pre/post central gyri), midbrain, and pontocerebellar white matter. Compared to those with PTSD, DID subjects showed increased FA in the right internal capsule and right temporal areas (predominantly implicating the inferior longitudinal fasciculus). Across DID and PTSD subjects, FA values within the aforementioned findings negatively correlated with depersonalisation, psychoform and somatoform dissociation, and/or traumatisation scores. Conclusions: Our DTI findings indicate markedly differential white matter integrity in DID compared to PTSD and HCs. This provides valuable mechanistic insights regarding a role for aberrant white matter structural integrity in traumatised female individuals with DID. https://pubmed.ncbi.nlm.nih.gov/39921931/
Data
Introduction
What is DID?
Definition - DID stands for dissociative identity disorder, one of three dissociative disorders recognised in the dms-5. DID is “a mental health condition where you have two or more separate personalities that control your behaviour at different times”. Each identity is almost like its own person, with different skills, ages, memories, interests, and so on. “DID reflects a failure to integrate various aspects of identity, memory, and consciousness into a single multidimensional self”. Cause - Dissociation is a result of intense stress or trauma; it’s the process of entering a mental state of detachment. During dissociation, people describe feeling intensely focused yet scarily detached from reality. Presentation - Some signs of DID include 2 or more distinct personality states (which may feel like possession), a loss of sense of self or self-agency, memory gaps in everyday life, forgetting personal information, and trouble recalling traumatic events that differ from normal (note that many of these symptoms are shared with other dissociative disorders). Somatic dissociation Prevalence - DID is a very rare condition, with 1.5% of the USA population being diagnosed with it, 1.4% of women and 1.6% of men.
Development
Everyone is born with multiple “behavioural states” which fuse at age 5/6 in normal childhood. In cases of abuse, that process is disrupted, and those states either stay separate, become increasingly independent, or split off into even more alters. Simply explained, if a child faces abuse that is too much for them to face alone and survive, their brain will use dissociation as a coping mechanism. When it comes to physical/sexual sensations, they are much harder to fully experience during dissociation. That makes it a good coping mechanism to mentally remove yourself from a situation when you can't physically. In the case of DID, while the “ANP” dissociates, an alter will take their place (see). While there is no known cause for DID, it is associated with the experience of traumatic events, abuse and/or overwhelming experiences during early development. Early signs of dissociation in children are problems with attachment, concentration, and memory. It is usually during adulthood when DID presents.
Alters
Identity
Identities often have separate roles, resulting in different skills, interests, behaviours, memories, assumed ages/sexes/ethnicities, etc., with the body often feeling as though it's undergone physical changes after switching. They also show psychobiological changes between alters, with differences in: ability, allergic responses, muscle tension, cardiovascular responses, regional cerebral blood flow, immune function, medication responses, and more.
ALTERS
There are two main types of alters: ANP (assumed normal parts), aka the host, and EP (emotional parts), who hold the traumatic memories and can often get caught up or stuck in them. The host is the one often presenting; they are in charge of daily basic functions, hiding the existence of all or some of the other alters from the world, and usually don't have any traumatic memories They are the alter presenting the vast majority of the time, and are what some might refer to as the “real person”, though all alters are part of the body's personality, and there is no one “real person”. In some cases, some alters will present through the ANP, temporarily blending with them. In ritual abuse cases, the ANP isn’t meant to be aware of the other alters. Each EP is created with a specific purpose. An EP is specially made to deal with a specific part of the abuse, but in some cases, EPs are groomed by abusers to perform the role they want them to. For example, a native american man described animal and spirit alters having been created through starvation, severe beatings, and hallucinogenic herbs/drugs. He developed a wolf alter as a result of being beaten for failure to commune with the wolf spirit. In usual cases, EPs allow the body to survive trauma in the moment and function afterwards. Most EPS are protective alters, though there are many kinds. Most protective alters are very defensive, push down emotions, and focus solely on protecting the body. There are prosecutor alters who act in a harmful way to protect the body. They often have a distorted view of reality and might intentionally hurt their bodies or others, thinking they’re being protective. For example, they might hurt the body in retaliation for a child alter disclosing specifics of the abuse in therapy, thinking they'll be hurt for opening up. Some perpetrators may be introjects of abusers, as discussed more in that section. They are “misguided protectors” but have protective and defensive intentions. Fight EP are another kind of protective alter, and like opresectors, they also have defensive intentions. “Fight” EPs aren’t always violent; they represent the fight part of PTSD. Gatekeeping alters are the alters present to experience the abuse, and the ones that hold it afterwards. This will keep the ANP from remembering the abuse and help them function afterwards. Internal self-help alters develop to help the body function with DID. They have an extensive understanding of the alters and system, and can help by explaining the system to a therapist. Caregiver alters are motherly alters that exist to take care of the body, alters, and sometimes even people outside of the system. They lack self-care and burn out easily, and they have limited capacity for leisure, as they are developed for this one specific role. The child alters, often nicknamed “littles” or “little ones,” are a very common EP. They often talk/ behave childishly, but can still have the cognitive function of an adult, but this isn't always the case. They usually exist to hold the traumatic memories from the ANP. Littles really vary, with some having a bubbly, childlike personality with one positive memory, while others hold onto the fear/pain of the trauma they carry, or some exist to show the “perfect child” of a “perfect “family. Dead alters, which are usually hidden from the rest of the system, are developed during experiences that felt like death to the alter. Alters aren't really able to die because, physically, they are more of a behavioural state than a separate being, so an alter can't actually die unless the brain dies. Introject alters are alters based on fictional or real people. They are rarely described by psychiatrists, except in ritual abuse cases. In military/political abuse cases, the alter may believe they are famous historical figures, or in religious abuse cases, the alter may believe they are a prominent religious figure. In political/military cases, the introject alter will often believe they are a bad person, such as a nazi or other war criminal, because they are a result of the abuse the body faced. The alter might believe they are the actual person, or there might be multiple alters believing theyre the same person, unaware of one another. People with these alters are often misdiagnosed with schizophrenia or a psychotic disorder. As treatment for these alters, their beliefs can change when given undeniable proof that they are not that person, since critical thinking and knowing are still there. These alters roles may be to keep loyalty to their abuser, which helps keep the body alive. Some intrpjects may believe they are the abuser, and they exist to “keep you in line” to protect from external abusers. They will often take on attributes of the abuser, such as beliefs or views, and will often verbally/physically abuse the body/system. They are a type of persecutor alter. Demon alters are a type of supernatural/spirit alters that often exist as a result of spiritual abuse or abuse that demonised the body. Some survivors report being forced to dress as a demon, then look in the mirror and be told that they are a demon, which can develop these alters. Disabled alters, alters who believe they have a physical disability that their body does not have, are often a result of instructions given by the abuser, such as “don’t talk”. They are a result of ïnvoluntary psycchsomatic symptoms, not a physical injury. This is a form of somatic dissociation, which is when psychological trauma creates physical symptoms instead of psychological ones. Animal alters are alters who believe that they are animals. They exist to express certain emotions that an ANP cannot. Some animals alters are predators that exist as a protector to the ANP when theyre distressed. Other alters exorcist as a result of abusers forcing children to act like animals, therefore they will think theyre the animal they were forced to act like. For example, if a child had to bark as communication or use a dog bowl for food, then they may develop a dog alter, or a snake alter, developing as a result of the child having movement restricted. Animal alters may also be a result of deep guilt from being forced to hurt others, because the harm they had to do may feel more violent than human, to the point of feeling animalistic. Animals can be taught that they are in a human body and therefore adapt. Non-Human alters are alters that believe they aren't human. While there are animal and supernatural alters, these alters aren't rooted in a belief that theyre a different creature; they believe they aren't human. Non-human alters are a result of severe dissociation, often from severe, long-term abuse that leaves the person feeling less than human. Opposite sex alters, who believe the body's sexual organs are different from what they actually are, may be a result of extreme dissociation, such as amnesia subtype, somatoform dissociation (which causes felt bodily sensations, ot of body experiences, and severe subconscious avoidance of the body. They are often not an accurate representation of that sex, but rather more of what a heterosexual might imagine the opposite sex. They often fit stereotypes of the opposite sex, such as female ones being timid/fearful, vs male ones being angry, physically strong or brave. Opposite gender alters believe they are a different person than the body was born as, but don't hold false beliefs about the body's anatomy. One way opposite sex/gender alters any development is through sexual trauwith For exampattemptede alter doesn't have a vaginthemnd therefore does not fear being vaginally raped, as the body was, or a female alter because the male body was forced to take on a female role while being raped, but not all opposite sex/gender alters are a result of sexual abuse. They may also fall into a different subtype of alters that believe they are in a different body than the rest of the system. Sexual alters exist to handle sexual abuse and hide that experience from the other alters. In some cases, one sexual alter may exist to take sexual abuse from women/girls, while another exists to take sexual abuse from men/boys. Suicidal or homicidal alters are very common. Not all alters who are suicidal/homicidal fall under this category, but these alters are often unaware that they share a body with the other alters, or believe that killing themselves will only harm them, not all the other alters. Over 70% of people with DID have attempted suicide, though not all of them have these alters.
Amount of alters
The amount of alters differs from person to person, depending on their traumatic experiences and their development. A 1984 study found that the majority of people with DID have between 2 and 100 alters, with 50% having 10 or fewer, and 50% having 11 or more. Women tend to have more, with an average of 15 alters per woman, and 8 per man. People usually uncover more alters they didn’t realise they had during treatment, with the average person having 2-4 known alters before treatment and finding another 13-15. This is because treatment gives alters a safe environment to make themselves and their experiences known.
Interaction
Switching is the process of going from one alter to another. People with DID describe becoming “suddenly depersonalised observers of their 'own” speech and actions, which they may feel powerless to stop” during/after switching . While one alter is present, they may hear the voices of the others, described as “multiple, perplexing, independent thought streams over which the individual experiences no control”. They might have sudden strong emotions, urges, or exhibit behaviours they hold personal ownership of. Preferences, interests and opinions suddenly switch from one to another, and many describe their bodies as feeling physically different.
Interidentity amnesia
Interidentity amnesia is amnesia between two states of consciousness (alters in DID). Sense of self is constructed by episodic and semantic autobiographical memories, therefore it is heavily impacted by personal encoding of stimuli. Personality is created of “modes” which have cognitive, affective, behavioural, and physiological ways of encoding information. In healthy controls, these modes all come together in the “conscious control system”, creating a more monolithic system. Different alters in DID draw upon and feel personal ownership over different memories, different parts of the same experience, and experiences with different narratives. These “owned” experiences/memories and their perceptions of them decide an identity's biologic factors, such as physiological arousal (heart/respiration rate, blood pressure), affective tone, and neurobiologic activation (brain activation). Interidentity amnesia occurs when information is encoded in a state of consciousness with its own psychobiological markers, then an attempt at retrieval is made in another state of consciousness, with extremely different biological markers. This means that amnesia will be particularly intense between two identities with especially different psychobiological makeup. Putamn's theory argues that trauma exposure leads to the development of “discrete behavioural states” which have a differing psychobiological makeup from other states of consciousness, leading to dissociative symptoms, and in extreme cases DID.
Solution
There is still a question about whether interidentity amnesia is cognitive, fully unable to retrieve, or metacognitive, its thought to be unretirveable and therefore becomes impossible. The metacognitive explanation explains cases where information is available between alters (at least in clinical settings). Metacognitive processes (metamemory in this case) monitor, control, and appraise memories to decide what is fit for goal-directed aims, assess subjective accuracy, control what information to use, and subjectively appraise the ability to remember. The metacognitive theory argues that interidentity amnesia is a result of metamemory processes rather than a deficit in memory functions. This may work in three different ways: alters believing information is inaccessible, and therefore gives up on their search for the information despite the availability, despite the information being retrived its believed not to be, or the retrieved information is believed to be foreign, and so the brain gets rid of it. In all, interidenity amnesia may be a distinct psychobiological difference between encoding states and retrieval states, but the solution may be trying to figure out how to bypass the belief that information is unretrievable, untrustworthy or foreign, thus leading to information being passed between alters.
Ritual abuse
Ritual abuse falls under the sub-section of organised abuse, a form of extremely sadistic and long-term abuse, along with network abuse, institutionalised abuse, and familial organised abuse. Ritual abuse groups are either religious/spiritual or political/military. Ritual abuse is “abuse that occurs in a context linked to some symbols or group activity that has a religious, magical or supernatural connotation, and where the invocations of these symbols or activities are repeated over time and used to frighten and intimidate the children”. It’s abuse that is long-lasting, intense, and tends to be physical, psychological, and sexual, while involving rituals of different types. Another description is “Repeated, extreme, sadistic abuse, especially of children, within a group setting. The group's ideology is used to justify the abuse, and the abuse is used to teach the group's ideology. The activities are kept secret from society at large, as they violate norms and laws” Due to the intensity and length of ritual abuse, many survivours develop DID later in life, with other survivours struggling with addiction, depression, anxiety, other dissociative disorders, C-PTSD, and bipolar disorder.
Alters in Ritual Abuse
Since ritual abuse is a part of organised crime, in many cases, the abuse is meant to give a person DID/develop a specific type of alter in them. Robot/machine alters are one common example of DID deliberately being given to someone/ a specific alter being deliberately developed in someone. These alters are under the belief that they are robotic, with no understanding of human emotion or the ability to feel their own. They are specifically groomed to follow orders and not think, with many believing they are physically unable to move unless being told to do so. Psychotic alters, alters who appear to have symptoms of psychosis, may be a result of ritual abuse. Alters may be groomed by abusers to have psychotic symptoms, usually to make a survivor's story less believable. It also might make it harder for the survivor to function or remember their abuse. Polyfragmented DID is classified as DID with 100 or more alters. These alters start as fewer and “split” into “fragments” of many alters that are very similar. When very severe trauma, such as ritual abuse, occurs, polyfragmented DID may be seen. Some alters behave as “partial” alters, either having little to no life story but a range of emotions, or little to no emotions but a complex life story. Some of these “paratextual” alters, called fragments, exist to play a very specific and limited role. For example, a fragment alter may exist to remember a very specific event. Another way that alters are groomed to perform certain roles is through alters who believe they’re fictional characters, fictives. In one case, a German survivor of ritual abuse during the Cold War had an alter groomed to believe he was Peter Munk, a character from a German fairytale who was “unemotional, obedient, and lacking in self-awareness”. This makes it easy to choose a character who fits all the criteria of the alter an abuser wants, then groom the victim into developing a fictive of them.
Life influences
Approximately 70% of people with DID have attempted suicide, with many more participating in self-harm behaviours. (Dissociative identity disorder (multiple personality disorder)) DID effects memory in three main ways; memory gaps with personal life events (important events such as death of a family member, birthdays, periods of time during childhood, ecvt.), lapses in “dependable memory” (evnts of the day, well-trained skills like reading, using a computer, doing ones job, ect.), and seeing evidence of tasks/ actionbs they dont remember doing (“coming to” in a place they domt remember going to (dissociative fugues), random items in their house, random injuries). Dissociative figues are very concerning, as you can “come to” in a place you don't want to be with no clue why or how to get back. DID's effects on function vary in intensity. For high-functioning people, DID tends to affect their relational functioning (marital, familial, parental), and not so much their occupational and professional life. DID can affect your functioning to the point where you may be unable to work, fully enjoy leisurely activities, and form deep platonic/romantic relationships, which can worsen the symptoms of the disorders associated with DID, such as worsening depression to the point of suicide or hospitalisation. DID affects everyone differently, according to gender and cultural differences. Females diagnosed with DID predominate among adult clinicians but not among pediatric clinicians. They present with acute dissociative states, e.g., flashbacks, amnesia, hallucinations, etc, more often than males. Males are more likely to deny their symptoms and trauma, leading to more false negative misdiagnoses of DID than women. They also show more criminal and violent behaviours than women. As DID is a trauma-based disorder, culture can have a big impact on the way it presents. In cultural settings where it's more normalised, we see more medically unexplained symptoms, such as non-epileptic seizures, paralysis, sensory loss, etc. Similarly, in cultural settings where possession DID is more normalised, we see increased rates of possession DID with non-human alters.
Validity of DID
Something heavily disrupted in the psychology world is the validity of DID. There are two main views: the sociocognitive model, which says DID is a result of high suggestibility, fantasy proneness, suggestive psychotherapy, and/or other suggestive sociocultural influences, and the position that DID is an extreme form of PTSD and just as valid as any other traumatic/dissociative disorder. The sociocognitive model argues that the guidelines for being diagnosed with DID are fairly simple to imitate: “(a) Behave as if you are two (or more) separate people who inhabit the same body. (b) Act as if the you I have been addressing thus far is one of those people and as if the you I have been talking to is unaware of the other co-inhabitants. (c) When I provide a signal for contacting another coinhabitant, act as though you are another person. To the extent that patients behave in terms of these rules, the “classic” symptoms [of DID] follow by implication and do not have to be taught through direct instruction or further suggestion”. This theory is supported by the correlation between fantasy proneness, suggestibility, susceptibility to pseudomemories and dissociative symptoms, but disproved by many biological/neurological factors of DID. The trauma related perspective, which is supported by countless psychological, physcobiological, and psychoneurological studies, is the theory stated in the DMS 5, and the basis of this project, argues that DID is the result of intense, prolonged sexual/physical trauma, usually beginning before the ages of 5/6, chronic emotional neglect, intense fear of primary caregiver(s), attachment disorders, and overall trauma disrupting the creation of a monolithic identity system. This view argues that DID is a severe form of PTSD, and acknowledges that DID patients can be influenced by sociocultural factors (as with many mental health disorders), false positive cases have been seen in higher amounts throughout the progression of DID research (it’s important to understand that the average person diagnosed with DID first has 12 years of inpatient care, receiving treatment for misdiagnoses, such as schizophrenia, BPD, BD, before being properly diagnosed/cared for, so false positives are few and far between), and that some psychiatric patients imitate DID (although major differences are seen between genuine and imitated DID. The official stance from the DMS 5 is that DID is a dissociative disorder and therefore an extreme form of PTSD.
Study
To prove the validity of the traumatic perspective of DID, analysizing a study comparing 11 DID patients, 10 high fantasy prone DID simulating controls (CH), and 8 low fantasy prone DID simulating controls (CL) by measuring subjective ratings (emotional/sensorimotor), automatic responses (heart rate and blood pressure), and regional cerebral blood flow (rCBF), which controls brain activation areas when NIS, TIS, CH, and CL while making sad and happy faces. The results showed Subjective results - in both sensorimotor and emotional results showed TIS much higher than all other controls, which all stayed in similar ranges. Heart rate results - The TIS showed the highest heart rate, NIS, and then the CH and CL, both being much closer to each other than the DID controls. Blood pressure (systolic and diastolic) results - TIS showed to be higher than the rest, which all stayed in the same range. rCBF results - while there were many areas of small change in the brain between DID controls and CH/CL, there was nowhere in specific where there were significant changes in rCBFbetween controls. The results of this study were that CL actually simulate DID better than CH. This disproves the sociocognitive theory, as brain activation/rCBF in CL simulates DID better than CH, concluding that there is a better connection between low fantasy proneness and DID than high fantasy proneness and DID.
Hippocampus
By comparing to AD, another disorder/disease that negatively affects the hippocampal volume, two main factors that go into decreasing hippocampal volume were found: a lack of neurogenesis and increased neural atrophy.
Adult neurogenesis
Adult neurogenesis is the process of neural stem cells (NSCs) proliferating, differentiating, and migrating, mainly in the hippocampus. They can develop into a variety of cells beneficial to the hippocampus, such as neurons, oligodendrocytes, and astrocytes. Differentiated neurons are essential to the organisation of complex circuits, processing information, transmission, consolidation, preservation, and organisation of memory, and regulating mood and behaviour. A lack of neurogenesis in the brain, specifically the hippocampus, will, of course, lead to a lower hippocampal volume. Increasing NSCs in the hippocampus could be a step towards a better treatment plan for DID. Three main methods to increase NSCs in the brain might be used: NSC transplantation therapy, NSC migration, and environmental/diet/exercise changes. Increasing hippocampal volume may help with DID symptoms such as memory issues, lack of emotional/behavioural problems, PTSD symptoms, interidentity amnesia, and it may help with dissociative symptoms (although the exact relationship between loss in hippocampal volume and dissociative symptoms is still unknown).
NSC transplantation therapy
NSC transplantation therapy is a promising pre-clinical therapy for diseases that affect the brain, being a treatment that can help the brain recover from neurodegenerative disease. It's currently being researched for use against amyotrophic lateral sclerosis (ALS), Parkinson’s disease (PD), Alzheimer's disease (AD) and Huntington’s disease (HD), but I believe that it could be an effective treatment for hippocampal volume loss seen in DID.
Method
NSCs can grow in single cell suspensions and form spherical clusters (neurospheres), which are non-adherent and can be “re-plated” to obtain neural cells. They can also be used to expand the pool of NSCs (for experimental or therapeutic purposes). Although an exact method to extract human tissue-derived NSCs has yet to be found, the technical methods would be similar to those of mammalian animals (which have been tested). If/when the method of NSC transplantation therapy is clinically validated, it may be a major development in the treatment of DID.
NSC migration therapy
They are reports of NSCs migrating from different parts of the brain (including the spinal cord, cerebral cortex and hippocampus). This could be a potential NSC therapy to increase hippocampal volume in the brain.
Stress exposure, diet and exercise
Stress exposure, exercise and diet all have a significant effect of nneurogenesis; cardio activity and a low calorie diet increase hippocampal neurogenesis, Omega 3 polyunsaturated fatty acids are essential to neuronal functioning as they have an anti flammatory effect, acute and chronic stress has seen to decrease adult neurogensis, reduce proliferation, neurogenerative cells, and the survival of new cells, and high fat diets decrease cell proliferation, survival, and increase apoptosis.
Neural atrophy
Neural atrophy is the destruction of neurons and their connections. The accumulation of Tdp-43 protein, β-amyloid, and tau in the amygdala accelerates hippocampal atrophy, so by stopping the accumulation of these in the brain, we can slow down neural atrophy. The nerve growth factor (NGF), neurotrophin 3 (NT-3), neurotrophin ⅘ (NT-⅘) and the brain derived neuro-trophic (BNDF) have all been seen to fight against neural atrophy. BNDF is a neurotrophin that protects neurons by promoting survival against neural insults. It's primarily sourced in neurons, astrocytes, and microglia. The reduction of BNDF in the brain leads to faster neural atrophy as cells have a decrease in protection. By increasing the NT -⅘, NT -3, BNDF, and NGF in the brain, we can protect pre-existing cells from neural atrophy, and by stopping the accumulation of Tdp-43 protein, β-amyloid, and tau in the amygdala, we can prevent the process of neural atrophy.
Hippocampal volume treatment plan
To increase hippocampal volume, it's been established that the treatment should involve increasing neurogenesis in the hippocampus and decreasing hippocampal atrophy. This can be done through potential NSC transplantation therapy, potentially migrating NSCs, lowering stress exposure, increasing exercise (specifically cardiovascular exercise), implementing a low-calorie diet (low in high fats (except omega 3)), increasing Neurotrophins in the CNS (specifically the hippocampus), preventing the accumulation of TDP-43 protien, β-amyloid, and tau in the amygdala, and earliest intervention possible. Increasing hippocampal volume may help with the following DID symptoms: memory deficits, interidentity amnesia, seizures, behavioural/emotional issues, PTSD symptoms, depressive symptoms, and overall functioning with DID.
Increasing neurogenesis
NSC transplantation therapy, though still in its pre-clinical state, is something that could be a great form of treatment for hippocampal volume loss seen in DID.
NSCs have been observed to migrate through the parenchyma across major distances to reach injury sites in the CNS (central nervous system). While the molecular mechanisms to manipulate NSC migration haven’t been developed, finding them and purposefully migrating NSCs to the hippocampus could be a promising treatment method for any disorder in which the hippocampus (or hypothetically any part of the CNS) shows a decrease in volume, including DID.
The treatment plan for the increase in hippocampal volume that could be tested now is decreasing stress exposure, increasing exercise, and keeping a low-calorie diet. By testing multiple patients with DID (or PTSD due to the small amount of DID patients and the psychologic and neurologic similarities seen between PTSD and DID) when they have the average diet/stress exporsure/excersize of a canadian with any severe mental health disorder, and comparing to patients with DID/PTSD who keep a low stress exporsure, a low calorie, high in Omega 3 diet, and a high amount of cardiovascular exercise over a period of time to measure changes in the hippocampal volume, overall brainhealth, and psychological symptoms seen in DID, then comparing the results, the effectiveness of this treatment method can be tested. There’s no harm in this experiment, although these conditions may be hard for the average DID patient to uphold, due to difficulty in reducing stress exposure, whether it’s enviromental or internal, affording/preparing healthy, low-calorie, high in Omega 3 food, and increasing exercise.
Decreasing neural atrophy
To increase BNDF in the hippocampus, taking antidepressants, SSRIs and TCAs, is an effective treatment. By medicating DID patients with SSRIs or TCAs, we may see help with DID symptoms, of course, but also PTSD and depressive symptoms, which may significantly help wth functioning.
Although research on increasing overall neurotrophins seems lacking, there has been research showing that long-term environmental enrichment increases neurotrophins in rats' brains. After rats were placed into either isolated conditions (IC), or environmental conditions (EC) for 1 month, starting at 2 months old, it was found that NGF and BNDF levels were increased in the cerebral cortex, hippocampal formation, basal forebrain, and hindbrain in EC rats, suggesting that that behavioural and neurological changes seen in relation to environmental stimulis has a biochemical basis. By having an enriched environment for those with DID, we may see increases in BNDF and NGF, leading to higher hippocampal and cerebral cortex volume, both of which have been seen to have a decrease in DID patients.
Though it was difficult to find information regarding the prevention of the accumulation of β-amyloid and tau in the CNS, information regarding reducing TDP-43 was found. In patients with neurodegenerative diseases, TDP-43 forms insoluble aggregates in the nucleus and cytoplasm of affected neurons instead of staying in its usual nuclear location. It's been shown that synthetic peptides could effectively inhibit the formation of TDP-43 protein aggregates in a concentration, but despite reducing the formation of TDP-43, the peptides did not reduce or prevent cell death. This means that there has yet to be an effective method for preventing cell death as a result of TDP-43 in neurodegenerative patients, but there are ways to increase and protect cells.
Non-epileptic siezures
Psychogenic non-epileptic seizures are episodes of movement, sensations, or behaviours similar to epileptic seizures that aren’t neurological in origin, but instead somatic manifestations of psychological distress. They are seen in especially high numbers in patients with DID, as comorbid psychiatric illness, notably depression, PTSD, somatoform disorders, dissociative disorders, as well as sexual and physical trauma history are all risk factors. To treat psychogenic non-epileptic seizures, the process is: creating a list of predisposing factors, then choosing a specific treatment plan. For patients with PTSD/dissociative symptoms, exposure therapies and serotonin reuptake inhibitors have been treatment plans in the past, as they work on the theory that psychogenic non-epileptic seizures are psychological in nature, and so will respond to psychiatric treatment.
Non-epileptic siezures
Treatment for DID/PTSD patients experiencing psychogenic non-epileptic seizures is to engage in exposure therapy, take SSRIs, and create a list of predisposing factors, then take a psychogenic approach to working through these factors.
Interidentity amnesia
Interidentity amnesia is amnesia between two states of consciousness (alters in DID). Sense of self is constructed by episodic and semantic autobiographical memories, therefore it is heavily impacted by personal encoding of stimuli. Personality is created of “modes” which have cognitive, affective, behavioural, and physiological ways of encoding information. In healthy controls, these modes all come together in the “conscious control system”, creating a more monolithic system. Different alters in DID draw upon and feel personal ownership over different memories, different parts of the same experience, and experiences with different narratives. These “owned” experiences/memories and their perceptions of them decide an identity's biologic factors, such as physiological arousal (heart/respiration rate, blood pressure), affective tone, and neurobiologic activation (brain activation). Interidentity amnesia occurs when information is encoded in a state of consciousness with its own psychobiological markers, then an attempt at retrieval is made in another state of consciousness, with extremely different biological markers. This means that amnesia will be particularly intense between two identities with especially different psychobiological makeup. Putamn's theory argues that trauma exposure leads to the development of “discrete behavioural states” which have a differing psychobiological makeup from other states of consciousness, leading to dissociative symptoms, and in extreme cases DID.
Meta-memory
There is still a question about whether interidentity amnesia is cognitive, fully unable to retrieve, or metacognitive, its thought to be unretirveable and therefore becomes impossible. The metacognitive explanation explains cases where information is available between alters (at least in clinical settings). Metacognitive processes (metamemory in this case) monitor, control, and appraise memories to decide what is fit for goal-directed aims, assess subjective accuracy, control what information to use, and subjectively appraise the ability to remember. The metacognitive theory argues that interidentity amnesia is a result of metamemory processes rather than a deficit in memory functions. This may work in three different ways: alters believing information is inaccessible, and therefore gives up on their search for the information despite the availability, despite the information being retrived its believed not to be, or the retrieved information is believed to be foreign, and so the brain gets rid of it. In all, interidenity amnesia may be a distinct psychobiological difference between encoding states and retrieval states, but the solution may be trying to figure out how to bypass the belief that information is unretrievable, untrustworthy or foreign, thus leading to information being passed between alters.
Treatment plan
If interidenity amnesia is meta-cognitive, by working on bypassing the belief that information is inaccessible, unhelpful or foreign, that should stop the metacognitive process, and increase functioning of not just ANPs (NIS), but also EPs (TIS), which not only would improve the quality of life for those with DID, but also increase the effectiveness of psychotherapy.
Grey matter and white matter volume
MRI scans from 17 patients with DID/co-morbid PTSD (DID-PTSD), 16 patients with PTSD only, and 32 healthy controls were analysed to compare their whole-brain cortical and sub-cortical grey matter morphological measurements. The grey matter in the brain makes up the outermost layer. Grey matter has a high neuron count, allowing for information processing and release. Relative to HC, patients with DID and PTSD showedlower volumes of cortical grey matter throughout their whole brain, specifically in their frontal, temporal, and insular cortices. Comorbid patients showed larger pallidum volumes and larger putamen and pallidum volumes relative to patients with PTSD only. Inconclusion, this study showed negative correlations between DID and cortical GM volumes in the whole brain, but positive correlations between DID and pallidum volumes.
65 female participants were in this study, 33 diagnosed with a trauma-related disorder, 17 of whom had DID. This study was done to measure the changes in white matter for patients with trauma-related disorders. White matter is brain matter found within the deep tissues of the brain. It has axons, extensions of neurons, that are often covered in Mylelin, giving it that white colour. White matter conducts, processes, and sends nerve signals up and down the spinal cord. (12, 13) All participants underwent DTI, diffusion tensor imaging, to measure the white matter in their brains. Patients with DID showed reduced white matter in their bilateral pallidum, midbrain, and pontocerebellar white matter. In conclusion, a negative correlation between DID and white matter is observed.
rCBF areas
The following graph shows the areas of abnormal brain activation in comparison to HC in NIS (neutral identity states) and TIS (traumatic identity states) The primary rCBf areas in TIS are;
| Cortical areas |
|---|
| Left and right Insula |
| Left orbitofrontal cortex |
| Left and right parietal operculum |
| Right Post/pre-central gyrus |
| Left and right Superior temporal gyrus |
| Subcortical areas |
| Left amygdala |
| Left candidate nucleus (anterior part, dorsal part, and tail) |
| Right candidate nucleus (caudal art, dorsal part, and lateral dorsal part) |
| Right putamen |
| Cerebullum |
| Left Cerebellar tonsil (nodule) |
| Right nucleus dentatus |
The primary rCBF areas in NIS are;
| Cortical areas |
|---|
| Right angular gyrus |
| Right anterior Cigluate gyrus |
| Right cingulate gyrus |
| Left and right cingulate sulcus |
| Left and right singulate sulcus |
| Left and right Cuneus |
| Right fusiform gyrus |
| Left inferior, medial, and medium frontal gyri |
| Right inferior, superior medial, and superior frontal gyrus |
| Eft and right superior frontal sulcus |
| Left and right lingual gyrus |
| Left middle and superior occipital gyrus |
| Right superior occipital gyrus |
| Left angular gyrus |
| Right occipitotemporal sulcus |
| Left and right parahippocampal gyrus |
| Right intra-parietal suluc |
| Left rostral inferior parietal lobule |
| Right superior parietal lobule |
| Left and right precuneus |
| Right recta gyrus |
| Left and right middle temporal gyrus |
| Subcortical areas |
| Left caudatus nucleus |
| Right lateral blobus pallidus |
| Right substantial nigra |
| Right thalamus |
| cerebelluem |
| Left cerebellum (anterior lobe) |
Psychologic symptoms
As a treatment for psychological symptoms, DID patients should engage in psychological therapy specific to DID/dissociative symptoms/PTSD.
Treatment
Current treatment
The main treatment is long-term psychotherapy in hopes of breaking down different identities to merge them into one, with other treatments including cognitive or creative therapies. There is no specific medication for DID, but antidepressants, anti-anxiety drugs, or tranquillisers can help reduce the psychological symptoms of DID. With the right treatment plan, those impaired by DID can have improvements in their personal and professional function.
Overall treatment plan
This treatment plan was created on the basis that by finding a way to decrease psychological symptoms, neurological changes, and proving the validity of DID, a new, more effective treatment plan can be widely implemented. The proposed treatment is: potential NSC transplantation therapy, potential NSC migration to the hippocampus (as well as other areas of the CNS affected in DID), decreasing stress exposure, increasing exercise (specifcally cardiovascular), keeping a low calorie diet, high in Omega 3 diet, SSRI medication, engaging in exposure based therapies for seizures, potentially working through metamemory processes therorictally seen in interidentity amnesia, maintaining an enriched enviroment, and engaging in psychotherapy specific to DID/dissociative symptoms/PTSD. This is an intensive treatment plan for DID that looks at the full picture of psychological, environmental, developmental, neurological, and biological factors of DID.
Case Studies
Louis Auguste Vivet, a Frenchman in the 19th century, was one of the first people on record to have DID. His attending physicians documented Vivet’s case during his time in the asylum. Vivet faced childhood abandonment, childhood abuse, adolescent homelessness, leg paralysis, a viper bite, and two asylum admissions. Vivet had psychological trauma from a snake bite, causing one of his alters to experience paralysis (add word). Another one of his alters was a thief as a result of having to provide for himself during his childhood years. He was sent to a rehabilitation centre at eight for these behaviours. At seventeen, he was sent to an asylum and released at eighteen, when he then went to visit his mother and work in agriculture. He was admitted back to an asylum after suffering a range of symptoms, ranging from complete paralysis to no symptoms. Oddly enough, while in paralysis, he was able to walk under “hypnosis” from an attending physician. He would have no memory of his stay at the asylum he went to at 17, but a complete recollection of his everyday life. He would report memory gaps with things changing before and after his gaps. He alternated between personalities, a thief, a griculturalist, so on. His symptoms of DID were reported as “a disruption of identity and episodic memory loss not caused by substance."12 — Surawijaya et al. (2023
An unnamed 55-year-old woman came into the general hospital with a history of substance abuse disorder, comorbid bipolar disorder, and fragmented personalities, under the influence of drugs and extreme stress. Her switches were infrequent and involuntary, though more frequent under the influence of drugs and emotional stress, causing the ANP intense emotional stress. She was documented to have increased violence during one-on-one visits compared to group visits. Her alters would act violently towards people, even loved ones, and cause homicidal and suicidal ideation, resulting in two past arrests. (check) She had four known alters; a seven year old girl, who was moody, arrogant, would sob or self harm if wants weren’t met, a teenager, who would increase the body’s substance abuse, alcohol use, and smoking, leading to multiple fights, homocidal attacks, and self harm attempts, a man, who would only act as an average man with heterosexual tendencies, male friends, and an assumed male body, and the ANP, a 55 year old woman. Her treatment was 6 months long, and it consisted of “psychotherapy with cognitive behavioural therapy addressing stress and substance use disorder”. She got drug treatment and was prescribed escitalopram to reduce anxiety symptoms (a disorder the ANP struggled with). While her condition was not drastically changed, her stress was improved.
Jeni Haynes, daughter of Richard Haynes, is an Australian woman with polyfragmented DID. Jeni developed 2500 distinct alters as a coping mechanism against the depraved abuse she suffered at the hands of her father. Richard was found guilty on 367 charges, including multiple accounts of rape, buggery, indecent assault, and carnal knowledge of a child under the age of 10. Jenis' abuse lasted 7 years, starting at age 3 and ending at 10 when her parents divorced, and her mother took custody. Of the six identities that testified, I could only find information on 3 of them. Muscles, an eighteen-year-old boy, tall with strong arms, who dresses like Billy Idol, is calm and protective. He gave physical evidence of the abuse Jeni suffered. Symphony, a four-year-old girl, was a gatekeeper to Jeni. "She suffered every minute of Dad's abuse, and when he abused me, his daughter Jeni, he was actually abusing Symphony," said Jeni. Symphony was Jeni’s first alter, who gave particulars of the abuse in court. Linda/Maggot, a tall, slender woman, “in a 1950s skirt with pink poodle appliqués, hair in an elegant bun with tapered eyebrows “. She gave a testimony to the academic and social impacts of Jeni’s abuse. She sought justice in 2009, but it was another 10 years before the police investigated.
Conclusion
In conclusion, using my research, a new, increasingly intensive treatment plan for DID has been created. The hypothesis that traumatic history affects the presentation/development of DID was proved correct, mainly through differences between TIS as a result of traumatic history. The hypothesis of DID negatively affecting the limbic system was also proven correct, with major volume loss in the hippocampus seen as a result of DID compared to HC and controls with BD, BPD, depression, and schizophrenia. The hypothesis of changes in blood pressure, heart rate, CNS activation areas, and blood flow between DIS, with a more fight/flight/freeze response seen in defensive TIS, was proved correct, with hyper arousal in the hippocampus when protective/defensive TIS are presenting. Seizures seen in DID patients has shown to be psychogenic non-epileptic seizures as a physical manifestation of intense stress, proving my hypothesis of seizures in DID being a result of stress correct. The hypothesis of the sociocognitive model of DID being disproved was proved correct, with the overwhelming evidence against it/for the traumatic view of DID. Though I don't have personal experience with DID, just from this extensive research, it is clear that DID is a completely debilitating disorder. Not just the disorder itself, but the way the public and mental health professionals treat it, and the lack of research into it. I once had a psychiatric nurse tell me that DID is a “misplacement of intelligence”. DID is a coping mechanism to prolonged, intense childhood sexual/physical trauma. It is something a person never fully, and for many, even partially, recovers from. Every time that you are able to go outside without fear of an alter taking over your body is something that people with DID don't get. Every time people take your health seriously. Every time you are able to work, enjoy your life, and form connections, it is something that a DID patient doesn't get, but it doesn't have to be this way. If we all work towards educating ourselves, taking DID seriously, stop alienating all mentally ill people, and start seeing them as fully human, not subhuman, not defective, not people who will never have any capacity to lead a good life, or who don't deserve to live a good life, but as fully human. People who can live a better life if we work for them. You have already helped by taking your time to understand this project, and so DID, now it’s your job to spread this message. Don't let people make jokes about “having multiple personalities”, don't let people alienate mentally ill people, and never forget that every person, regardless of mental state, is human and equal to anybody else. I hope that I can truly test out my treatment plan, and if given the chance, I will not stop until I’ve been able to help in some way.
Citations
Hippocampal Research
Hippocampus | definition\, location\, function\, & facts | britannica. (n.d.). https://www.britannica.com/science/hippocampus Cantu, R. C. (2001, September). Posttraumatic retrograde and Anterograde amnesia: Pathophysiology and implications in grading and safe return to play. Journal of athletic training. https://pmc.ncbi.nlm.nih.gov/articles/PMC155413/ Rao, Y. L., Ganaraja, B., Murlimanju, B. V., Joy, T., Krishnamurthy, A., & Agrawal, A. (2022, February 1). Hippocampus and its involvement in alzheimer’s disease: A review - 3 biotech. SpringerLink. https://link.springer.com/article/10.1007/S13205-022-03123-4 Chalavi S;Vissia EM;Giesen ME;Nijenhuis ER;Draijer N;Cole JH;Dazzan P;Pariante CM;Madsen SK;Rajagopalan P;Thompson PM;Toga AW;Veltman DJ;Reinders AA; (n.d.). Abnormal hippocampal morphology in dissociative identity disorder and post-traumatic stress disorder correlates with childhood trauma and dissociative symptoms. Retrieved from https://pubmed.ncbi.nlm.nih.gov/25545784/ Professional, C. C. medical. (2025). Hippocampus: What’s its function? Retrieved from https://my.clevelandclinic.org/health/body/hippocampus
Neural stem cell therapy
Tang, Y., Yu, P. & Cheng, L. Current progress in the derivation and therapeutic application of neural stem cells. Cell Death Dis 8, e3108 (2017). https://doi.org/10.1038/cddis.2017.504
Neural stem cell migration
J. Imitola,K. Raddassi,K.I. Park,F. Mueller,M. Nieto,Y.D. Teng,D. Frenkel,J. Li,R.L. Sidman,C.A. Walsh,E.Y. Snyder, & S.J. Khoury, Directed migration of neural stem cells to sites of CNS injury by the stromal cell-derived factor 1α/CXC chemokine receptor 4 pathway, Proc. Natl. Acad. Sci. U.S.A. 101 (52) 18117-18122, https://doi.org/10.1073/pnas.0408258102 (2004).
Neurotrophins
Carl Björkholm, Lisa M. Monteggia, BDNF – a key transducer of antidepressant effects, Neuropharmacology, Volume 102, 2016, Pages 72-79, ISSN 0028-3908, https://doi.org/10.1016/j.neuropharm.2015.10.034. (https://www.sciencedirect.com/science/article/pii/S002839081530157X) Ickes, B. R., Pham, T. M., Sanders, L. A., Albeck, D. S., Mohammed, A. H., & Granholm, A. C. (2000). Long-term environmental enrichment leads to regional increases in neurotrophin levels in rat brain. Experimental neurology, 164(1), 45-52.
Grey Matter Research
Wise, T., Radua, J., Via, E., Cardoner, N., Abe, O., Adams, T. M., Amico, F., Cheng, Y., Cole, J. H., de Azevedo Marques Périco, C., Dickstein, D. P., Farrow, T. F. D., Frodl, T., Wagner, G., Gotlib, I. H., Gruber, O., Ham, B. J., Job, D. E., Kempton, M. J., … Arnone, D. (2016, May 24). Common and distinct patterns of grey-matter volume alteration in major depression and bipolar disorder: Evidence from Voxel-based meta-analysis. Nature News. https://www.nature.com/articles/mp201672#Sec5 Chalavi S;Vissia EM;Giesen ME;Nijenhuis ER;Draijer N;Barker GJ;Veltman DJ;Reinders AA; (n.d.). Similar cortical but not subcortical grey matter abnormalities in women with posttraumatic stress disorder with versus without dissociative identity disorder. Retrieved from https://pubmed.ncbi.nlm.nih.gov/25670646/ Mercadante, A. A. (2023). Neuroanatomy, gray matter. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK553239/ Team, Spinalcord. com. (2020a). Grey matter vs white matter in the brain. Retrieved from https://www.spinalcord.com/blog/gray-matter-vs-white-matter-in-the-brain
White matter
White matter of the brain: Medlineplus medical encyclopedia. (n.d.). Retrieved from https://medlineplus.gov/ency/article/002344.htm Team, Spinalcord. com. (2020a). Grey matter vs white matter in the brain. Retrieved from https://www.spinalcord.com/blog/gray-matter-vs-white-matter-in-the-brain Dimitrova LI;Chalavi S;Vissia EM;Barker GJ;Perez DL;Veltman DJ;Diez I;Reinders AATS; (n.d.). Brain white matter structural connectivity of trauma and trauma-related dissociation disorders and symptoms. Retrieved from https://pubmed.ncbi.nlm.nih.gov/39921931/
Non-epileptic Seizures
Alsaadi, T. M., & Marquez, A. V. (2005, September 1). Psychogenic nonepileptic seizures. American Family Physician. https://www.aafp.org/pubs/afp/issues/2005/0901/p849.html#treatment
Psychobiology Research
Reinders, AAT Simone, et al. "Psychobiological characteristics of dissociative identity disorder: a symptom provocation study." Biological psychiatry 60.7 (2006): 730-740. Şar, Vedat, Martin J. Dorahy, and Christa Krüger. "Revisiting the etiological aspects of dissociative identity disorder: a biopsychosocial perspective." Psychology research and behavior management (2017): 137-146.
Validity of DID as a form of PTSD
Reinders AA, Willemsen AT, Vos HP, den Boer JA, Nijenhuis ER. Fact or factitious? A psychobiological study of authentic and simulated dissociative identity states. PLoS One. 2012;7(6):e39279. doi: 10.1371/journal.pone.0039279. Epub 2012 Jun 29. Erratum in: PLoS One. 2012;7(7): doi/10.1371/annotation/4f2000ce-ff9e-48e8-8de0-893b67efa3a4. Reinders, A A T Simone [corrected to Reinders, A A T S]. PMID: 22768068; PMCID: PMC3387157.
What is DID (overview)
Dissociative identity disorder (DID). (2025). Retrieved from https://my.clevelandclinic.org/health/diseases/9792-dissociative-identity-disorder-multiple-personality-disorder Dissociative identity disorder (multiple personality disorder). (n.d.). Retrieved from https://www.psychologytoday.com/ca/conditions/dissociative-identity-disorder-multiple-personality-disorder (Dissociative identity disorder (DID) DSM5 code 300.14 (ICD-10 F44.81))
Alters in DID
van der Hart, N. & K. S., & Traumadissociation.com. (2016). Alter identities in dissociative identity disorder (MPD), OSDD and P-did. Retrieved from https://traumadissociation.com/alters.html (Jan 12, 2026). Traumadissociation.com. Retrieved Jan 25, 2026, from https://traumadissociation.com/other
Ritual Abuse
Raschke, C., Bass, E., Davis, L., Nathan, D., Snedeker, Force, R. A. T., & BBC. (1994b). Ritual abuse: Satanic ritual abuse, MKUltra, convictions, myths and facts. Retrieved from https://traumadissociation.com/abuse/ritual-abuse-mkultra-satanic-panic-vs-facts.html
Case Studies
Rehan MA;Kuppa A;Ahuja A;Khalid S;Patel N;Budi Cardi FS;Joshi VV;Khalid A;Tohid H; (n.d.). A strange case of dissociative identity disorder: Are there any triggers? Retrieved from https://pubmed.ncbi.nlm.nih.gov/30214845/ Mao, F. (2019a). Dissociative identity disorder: The woman who created 2,500 personalities to survive. Retrieved from https://www.bbc.com/news/world-australia-49589160
Images
Reinders, A. A. T. S., Marquand, A. F., Schlumpf, Y. R., Chalavi, S., Vissia, E. M., Nijenhuis, E. R. S., Dazzan, P., Jäncke, L., & Veltman, D. J. (2018, December 7). Aiding the diagnosis of dissociative identity disorder: Pattern recognition study of brain biomarkers: The British Journal of Psychiatry. Cambridge Core. https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/aiding-the-diagnosis-of-dissociative-identity-disorder-pattern-recognition-study-of-brain-biomarkers/DCF85A7D69652C06E61524593B266E8C (N.d.-b). Enigma’s large-scale studies of nine brain disorders. Cortical Gray... | download scientific diagram. (n.d.-a). https://www.researchgate.net/figure/ENIGMAs-Large-Scale-Studies-of-Nine-Brain-Disorders-Cortical-gray-matter-thickness_fig3_334232733
Header Image
Reinders, A. A. T. S., Marquand, A. F., Schlumpf, Y. R., Chalavi, S., Vissia, E. M., Nijenhuis, E. R. S., Dazzan, P., Jäncke, L., & Veltman, D. J. (2018, December 7). Aiding the diagnosis of dissociative identity disorder: Pattern recognition study of brain biomarkers: The British Journal of Psychiatry. Cambridge Core. https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/aiding-the-diagnosis-of-dissociative-identity-disorder-pattern-recognition-study-of-brain-biomarkers/DCF85A7D69652C06E61524593B266E8C
Acknowledgement
Pediatric psychiatric nurse Anthony: Thank you for giving me your opinion on DID, saying that it was a “misplacement of intelligence”. Not only did he give me a window into the medical view of DID, but he also encouraged me to prove him wrong. Without him, I wouldn’t have looked at the psychobiological aspects of DID or the medical view of DID. Camille Jasper: Thank you so much mom for listening to me talk about the science fair for hours and actually being interested. Thank you to all the teachers at my school who worked together to let so many students do the science fair. Thank you to all the sponsors of CYSF for giving kids all around Calgary this opportunity.