”Immuni-Mama” - Risk Severity Assessment Model for Pregnant Women with Inborn Errors of Immunity and Secondary Immunodeficiency
Eileen Niftaliyeva, Inga Deryabina
Western Canada High School
Grade 11
Presentation
No video provided
Problem

Abstract
Intro: Immunocompromised pregnant women are at increased risk of infections, including urinary tract, respiratory, and gastrointestinal infections, which may contribute to adverse outcomes such as preterm birth, fetal growth restriction, and stillbirth. There is not available tool available for earlier identification of clinically significant (most common) infections in immunodeficient pregnant women by systematically assessing reported symptoms and relevant medical history. There is a limited amount of published research related to infection risk in immunodeficient patients. We aimed to build this model as a supervised model using the publicly available data and literature.
Methods: Based on a detailed literature reviewed we extracted essential data to develop a model. Model description. Given that this is a supervised simulated model we can only talk about internal validation, not accuracy. We set hypotheses with respect to medical conditions of the pseudo patients
Results: We developed a Risk Severity Assessment Model for Pregnant Women with Inborn Errors of Immunity and Secondary Immunodeficiency. This model is designed to estimate risk of unfavourable pregnancy results for both the immunocompromised women and the fetus, allowing to recognize warning signs of the most common infections found characterizing the respective immunodeficiency and advising the user when urgent clinical consultation is needed.
The risk severity assessment model (Infection Severity Screening Framework) is designed to estimate risk of unfavourable pregnancy results for both the immunocompromised women and the fetus, allowing to recognize warning signs of the most common infections found characterizing the respective immunodeficiency and advising the user when urgent clinical consultation is needed. We hypothesize that we can build this model as a supervised model using the publicly available data and literature. Given that this is a supervised simulated model we can only talk about internal validation, not accuracy. We set hypotheses with respect to medical conditions of the pseudo patients. The model can be potentially integrated into a patient or doctor-facing digital tool (and we are building the proof-of-concept of this tool as a part of our project). This tool will support earlier identification of clinically significant (most common) infections in immunodeficient pregnant women by systematically assessing reported symptoms and relevant medical history. By providing structured risk stratification and clear guidance on when to seek medical care, the application aims to empower pregnant women in the decision-making process and reduce the risk of adverse maternal and fetal outcomes. Also, since this topic has not been extensively researched (and also there is some complexity associated with privacy which makes assess to some data impossible to us), there is a possibility that we won’t be able to access high quality data and thus we’ll have to determine odds ratio for risk factors and weight of alert sights based on the clinical criteria rather than on predictions generated based on our training data set.
Introduction / Background
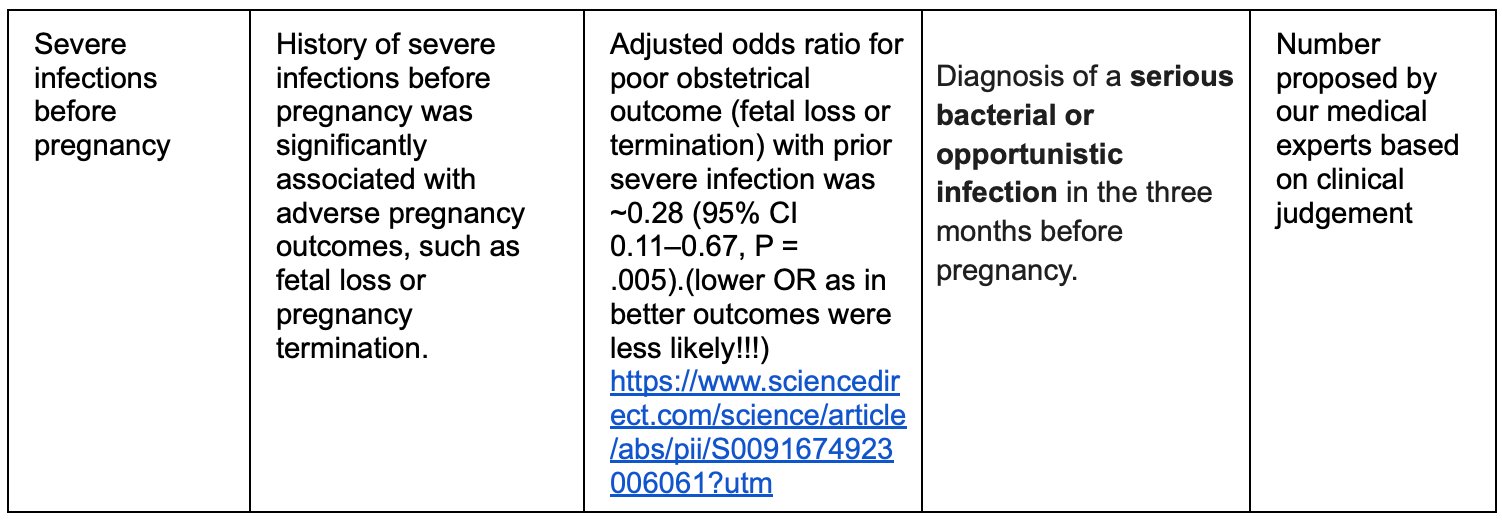
Immunocompromised pregnant women are at increased risk of infections, including urinary tract, respiratory, and gastrointestinal infections, which may contribute to adverse outcomes such as preterm birth, fetal growth restriction, and stillbirth.[1] In pregnant women with Inborn Errors of Immunity (Primary immunodeficiency), history of severe or recurrent infections and inadequate antimicrobial prophylaxis has been associated with worse pregnancy outcomes (odds ratio 0.28, 95% CI 0.11–0.67, p=0.005), although estimates remain imprecise due to small sample sizes. [2] Particularly significant antibody deficiencies and combined immunodeficiencies, are associated with higher infection risk during pregnancy and, consequently, increased risk of complications.[3]
Women with secondary immunodeficiency, particularly those with systemic lupus erythematosus (SLE) who received immunosuppressive therapy, also experience elevated maternal and fetal risks. In the PROMISSE cohort, 15% of women with SLE developed preeclampsia, increasing to 22% among those with antiphospholipid antibodies.[4]
The risk of severe infections, including sepsis and pneumonia, is further increased due to both immune dysregulation and immunosuppressive therapy. Dose-response analyses have demonstrated higher incidence rates of serious infections among pregnant women treated with systemic corticosteroids compared with other immunosuppressive regimens.
Despite this elevated infection risk in immunocompromised pregnant women, there are currently no practical tools with warning signs that could support early detection of severe infections based on symptom assessment and medical history.
Other logistics predictive models we reviewed with a high accuracy rate[5,6,7]:
The First Trimester Preeclampsia Screening Algorithm, is a logistics model developed by the FMF in Austria to find Preeclampsia in pregnant women based on their symptoms, with an accurate rate of 90% for early-onset PE, 75% for preterm PE, and a 10% false-positive rate as analyzed by source [8].
The model Framingham Risk Score for Hard Coronary Heart Disease, is a logistics model that predicts an individuals 10 year risk for coronary heart disease, with a >80 accuracy.[9,10]
CHA₂DS₂-VASc Score for Atrial Fibrillation Stroke Risk, predicts patients with atrial fibrillation risk of stroke with an accuracy of \~80.[11,12]
Purpose / Objective
Our goal is to use published clinical data to develop a prediction model that supports immunocompromised pregnant women in recognizing warning signs of common infections and determining when urgent clinical consultation is warranted. Earlier detection of clinically significant infections may improve maternal safety and reduce the risk of pregnancy loss, fetal growth restriction, and impaired fetal development. Based on this model, we wanted to design and develop a prototype mobile application to ensure practical applicability and accessibility for the target population. Recognizing the importance of usability in digital health tools, our objective at this stage is not only to refine the underlying risk model but also to evaluate the user interface and user experience (UI/UX). Although the current project timeline does not allow for full clinical validation, we aim to collect early user feedback to assess feasibility, acceptability, and usability, which will inform further development and future validation studies.
Hypothesis
Based on the available literature/data, we can: Identify the critical risk factors for most common types of immunodeficiency that would lead to pregnancy failure. Identify the alert signs that would indicate a high risk of pregnancy failure Identify statistically significant associations that allow us to calculate odds ratios (OR) for key risk factors, along with their confidence intervals and p-values. Similarly, for alert signs (symptoms), extract values indicating their clinical significance and predictive strength in relation to infection severity in high-risk pregnancies. Build a prediction model - Infection Severity Screening Framework, that can be potentially integrated into a mobile application. This tool will support earlier identification of clinically significant infections in immunodeficient pregnant women by systematically assessing reported symptoms and relevant medical history. By providing structured risk stratification and clear guidance on when to seek medical care, the application aims to empower pregnant women in the decision-making process(as well as physicians) and to support a reduction in the risk of adverse maternal and fetal outcomes.
Method

Materials
- Literature review and extraction of information about: the most common infections in immunodeficient pregnant women, the analysis of critical symptoms and their duration and their role in the severity of infections and risk for poor pregnancy outcomes, statistical correlation between severity of infections and medical background.
- Evaluate the quality of available data and modify our “risk factors -> alert signs” maps accordingly. Build the predictive model out of this data. The model will be based on the simulated data since the complete data is not available, but in the future we are planning to obtain the real data from the patients.
List all equipment, tools, and resources used
- Medical literature platforms: Ncbi, Pubmed
- Interviews with specialist
- Mobile app development toolkit: Android studio. Kotlin Multiplatform
- Data science toolkit: ML libraries, Python
-
Cloud backend: AWS
-
Method/Procedure Key concepts/terms Risk Factors Pre-existing or currently existing conditions and environmental factors that increase the probability of pregnancy failure in immunocompromised women. Risk factors are categorized by their rate of change: Static Risk Factors: Unchangeable or nearly unchangeable characteristics that remain constant throughout pregnancy (e.g., maternal age, genetic markers, permanent medical conditions). These factors are established at baseline and do not vary during the pregnancy timeline. Semi-static Risk Factors: Conditions that may change gradually over extended periods, typically months rather than weeks (e.g., immunoglobulin levels, slowly evolving chronic conditions). While not fixed, these factors demonstrate relative stability during pregnancy. Dynamic Risk Factors: Conditions or environmental factors that can change more frequently and actively influence pregnancy outcomes (e.g., active infections, which begin as environmental exposures and become ongoing risk factors). Unlike alert signs, these are the risk-increasing conditions themselves, not their manifestations.
Risk Factors
Pre-existing or currently existing conditions and environmental factors that increase the probability of pregnancy failure in immunocompromised women. Risk factors are categorized by their rate of change:
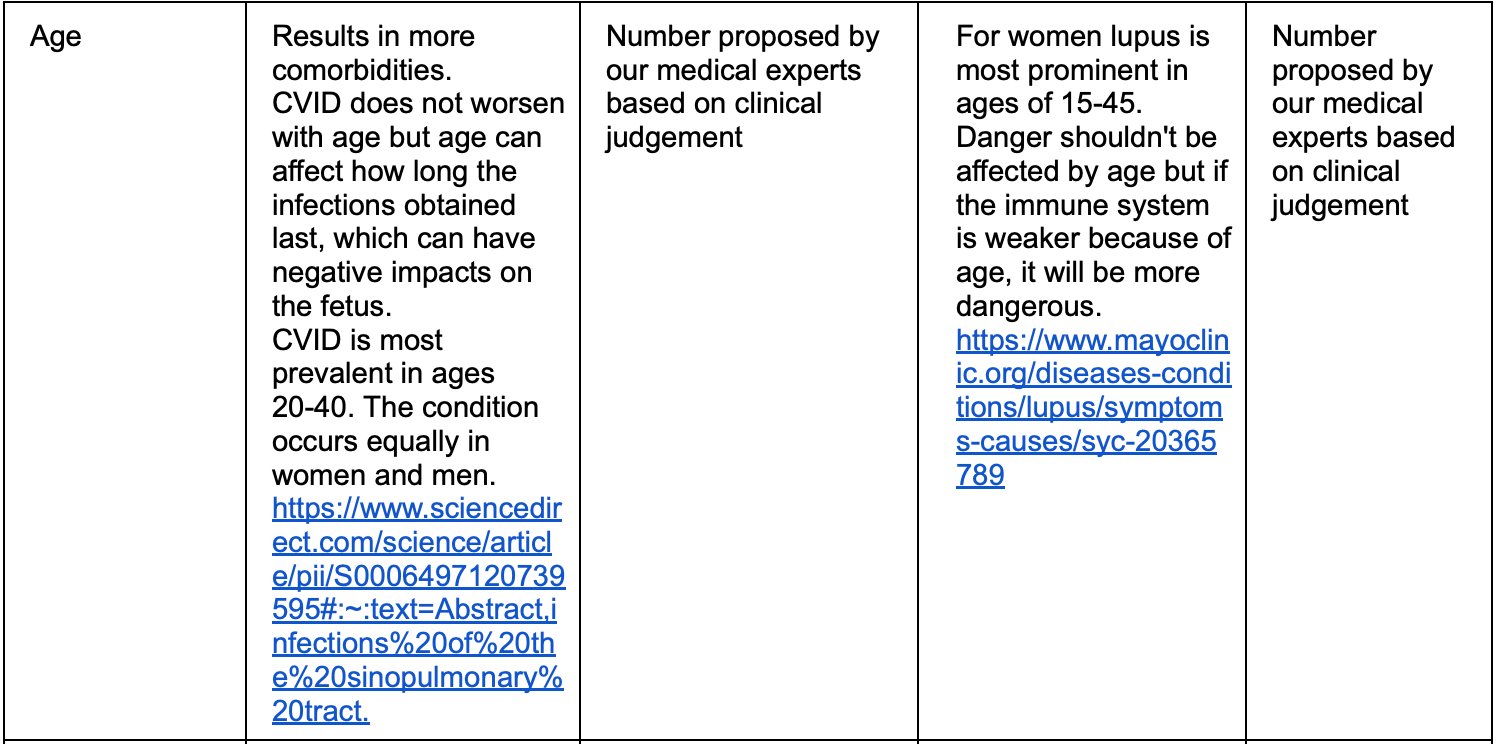
- Static Risk Factors: Unchangeable or nearly unchangeable characteristics that remain constant throughout pregnancy (e.g., maternal age, genetic markers, permanent medical conditions). These factors are established at baseline and do not vary during the pregnancy timeline.
- Semi-static Risk Factors: Conditions that may change gradually over extended periods, typically months rather than weeks (e.g., immunoglobulin levels, slowly evolving chronic conditions). While not fixed, these factors demonstrate relative stability during pregnancy.
Dynamic Risk Factors: Conditions or environmental factors that can change more frequently and actively influence pregnancy outcomes (e.g., active infections, which begin as environmental exposures and become ongoing risk factors). Unlike alert signs, these are the risk-increasing conditions themselves, not their manifestations.
Odds Ratio
A statistical metric derived from published medical literature that quantifies the magnitude of risk associated with each risk factor. The odds ratio indicates how many times more (or less) likely pregnancy failure becomes when a specific risk factor is present, providing an evidence-based measure of each factor's contribution to overall risk.
Alert Signs
Measurable or noticeable indicators that signal the risk of pregnancy failure is manifesting or changing. Unlike risk factors, which increase the probability of failure, alert signs are observable symptoms or clinical measurements that demonstrate the risk is actively materializing. Alert signs serve as real-time warnings that intervention may be needed.
Weights
A significance metric assigned to each alert sign, developed by medical experts through analysis of clinical data rather than derived from published literature. Weights quantify the clinical importance and urgency of each alert sign, reflecting expert judgment about which indicators most strongly signal imminent pregnancy complications in immunocompromised patients. For simplicity and unification, we converted odds ratio to weights for risk factors too.
Methods
We explored published data on the relationship between infection severity and key clinical variables, including duration of symptoms, trimester of pregnancy, pre-existing treatment regimens including supportive treatment (prophylactic antibacterial/antifungal treatment, immunoglobulin replacement therapy) and immunosuppressive treatment (rituximab, steroids), comorbid conditions and social factors.
We conducted a comprehensive literature review analyzing the risk factors affecting pregnant women with inborn errors of immunity (IEI) and secondary immunodeficiency. We explored published data on the relationship between infection severity and key clinical variables, including duration of symptoms, trimester of pregnancy, pre-existing treatment regimens, and comorbid conditions.
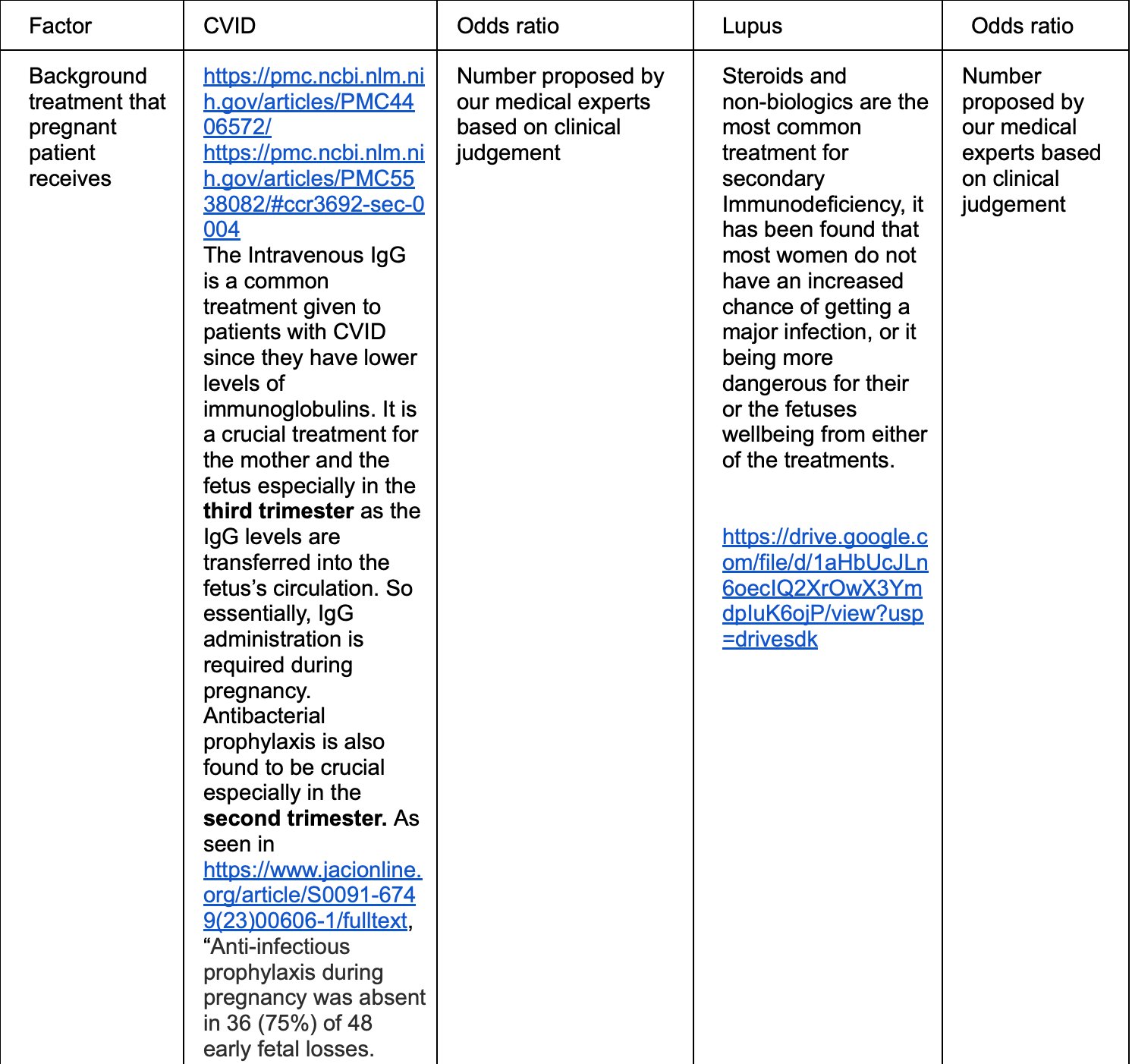
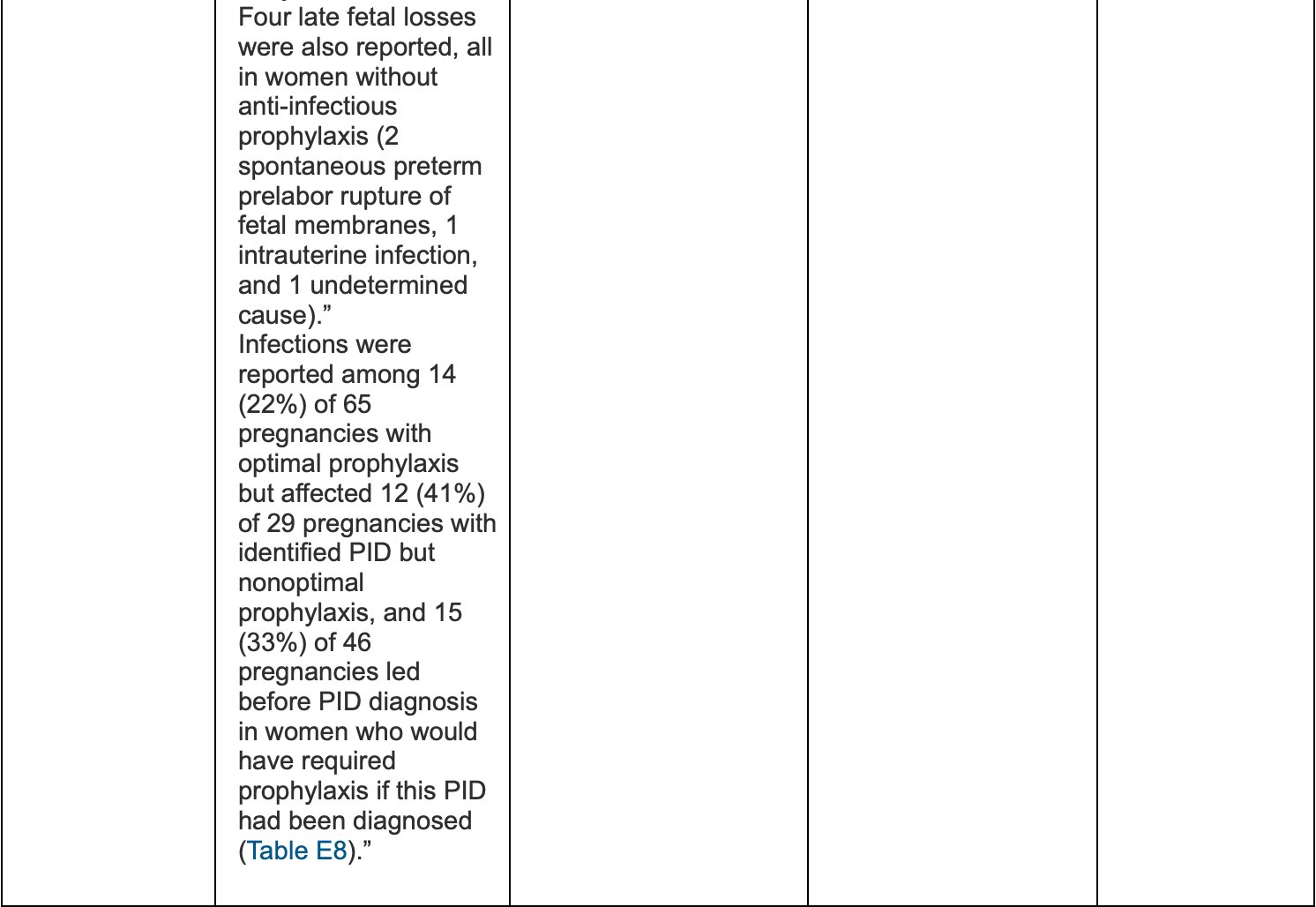
I group: In analyzing available studies on pregnant women with IEI, we focused particularly on cohorts with primary antibody deficiencies. We extracted data regarding infection frequency during pregnancy, use of prophylactic therapies (antibacterial and antifungal), and administration of immunoglobulin replacement therapy. However, detailed descriptions of infection-related symptoms during pregnancy were limited in the literature. To address this gap, we incorporated published data describing clinical manifestations of infections in non-pregnant women with common variable immunodeficiency (CVID) to inform symptom weighting and model development. Notably, published research specifically addressing pregnancy outcomes and infection characteristics in women with IEI remains limited.[13]
Currently, there are more than 500 IEIs - rare diseases registered according to the classification of International Union of Immunological Societies (IUIS). Evaluation of risk factors of severe infections for pregnant women with various IEIs requires further research.[14]
II group: We also conducted a focused literature review of pregnant women with secondary immunodeficiency receiving immunosuppressive therapy for autoimmune diseases, particularly systemic lupus erythematosus.[15] We examined the types of immunosuppressive agents used and their association with infection risk, with specific attention to corticosteroids and biologic therapies, including rituximab.
Primary Immunodeficiency (PID - Focused on Common Variable Immune Deficiency - CVID) Type of Immunodeficiency: Specific PID types, such as significant antibody deficiencies or combined immunodeficiencies, which carry a higher infection risk and thus a higher probability of complications. Medical History: A history of severe, recurrent infections before pregnancy and inadequate antimicrobial prophylaxis. Prior Procedure: A previous maternal splenectomy (particularly for women with primary immune thrombocytopenia, a related condition) is associated with neonatal thrombocytopenia. Specific Subtype Outcomes (IgA deficiency): Increased risk of Small for Gestational Age (SGA) Birth and Cesarean Section. Secondary Immunodeficiency (SID - Associated with Systemic Lupus Erythematosus - SLE, and other autoimmune/immunosuppressive conditions)
Underlying Conditions & Disease Activity:
Autoimmune Conditions:
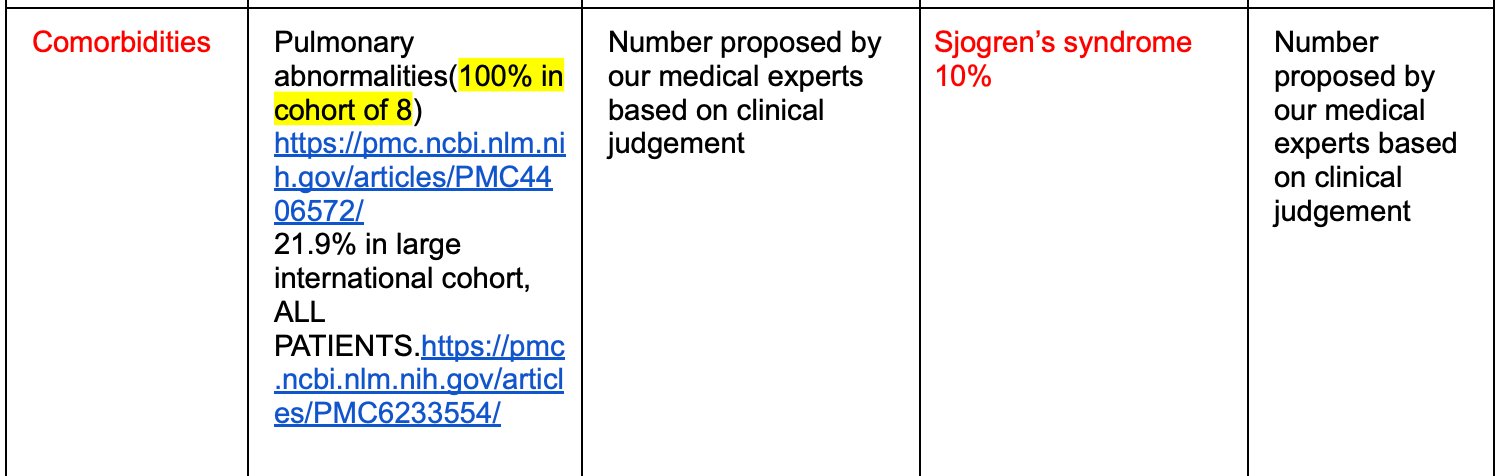
Systemic Lupus Erythematosus (SLE), Rheumatoid Arthritis, Ankylosing Spondylitis, Psoriatic Arthritis, or Inflammatory Bowel Disease.[21] High disease activity of the autoimmune condition during pregnancy. The presence of positive Antiphospholipid Antibodies (aPL), which increases the risk of pre-eclampsia in women with SLE and is associated with 10% of pregnancy losses at 20 weeks in Antiphospholipid Syndrome (LPS/aPL).[22,23]
Other SID-Causing Conditions: HIV, Types of cancer, Sickle cell disease, Viral hepatitis, and Liver cirrhosis.
Prior Infection History: Diagnosis of a serious bacterial or opportunistic infection in the three months before pregnancy.
Treatment-Related Factors:
- High-Dose Steroids: Higher average daily dose of systemic steroids during pregnancy is identified as an independent risk factor for serious infections.
- Immunosuppressive Agents: Use of any immunosuppressive drug class, including systemic steroids, non-biologic agents, or TNF inhibitors (the study found similar risk of serious infections across these classes, but they are all considered risk factors due to their function).
Below are the overview of the most important risk factors (static, semi-static and dynamic) we identified based on the literature review and experts interviews.
- Static and semi-static risk factors
Based on the literature review[17,18,19], the key pre-existing risk factors affecting pregnancy for primary and secondary immunocompromised women are:
- Immunodeficiency mechanism: type of inborn error of immunity or secondary immune deficiency
- Age of Pregnant women
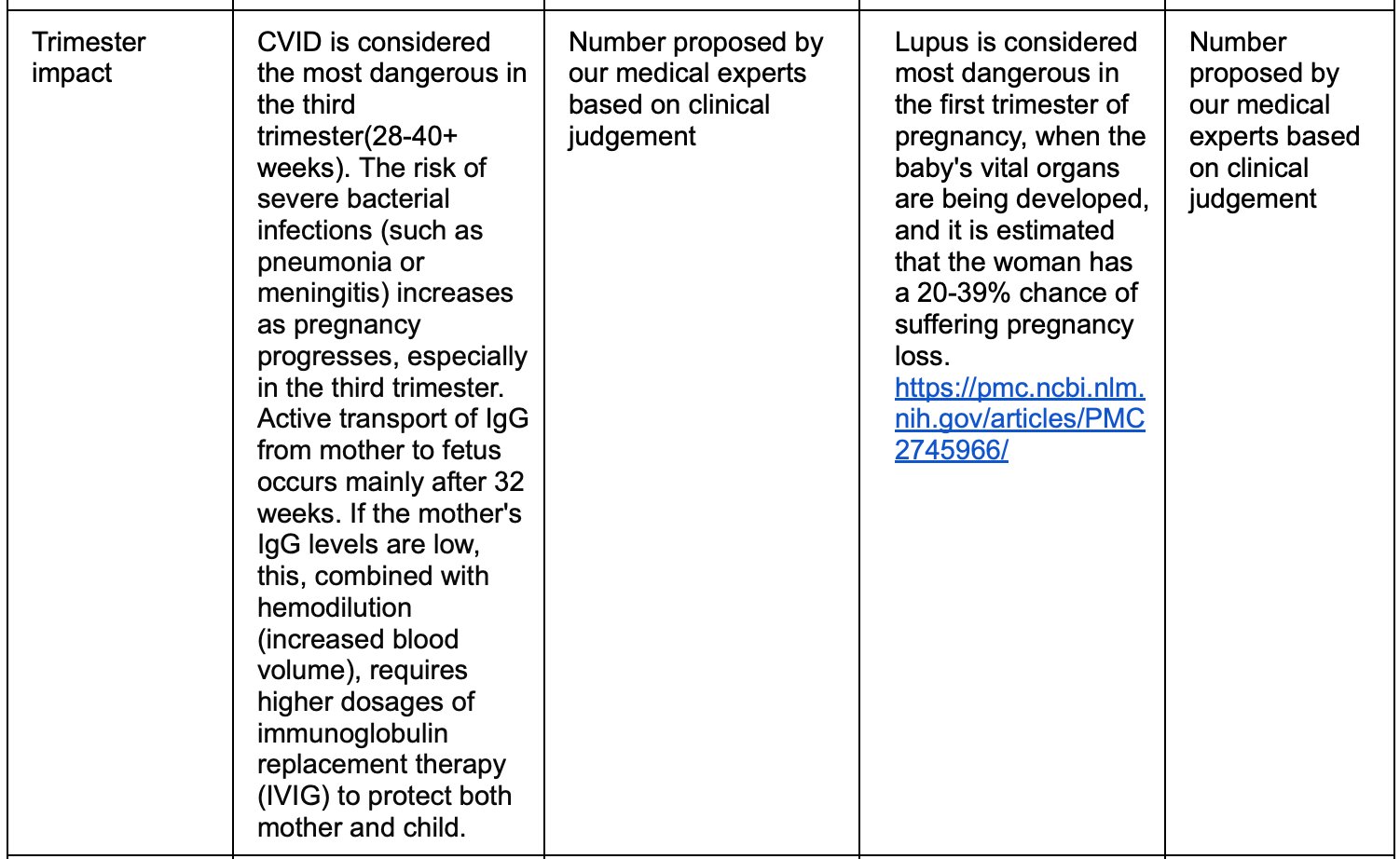
- Trimester of pregnancy: I, II, III
- Medical History: A history of severe, recurrent infections before pregnancy and inadequate antimicrobial prophylaxis.
- Treatment:
- a. supportive treatment: IVIG, antibacterial/antifungal prophylaxis,
- b. immunosuppressive treatment: steroids, Rituximab, Infliximab or other biologics, other immunosuppressive medications
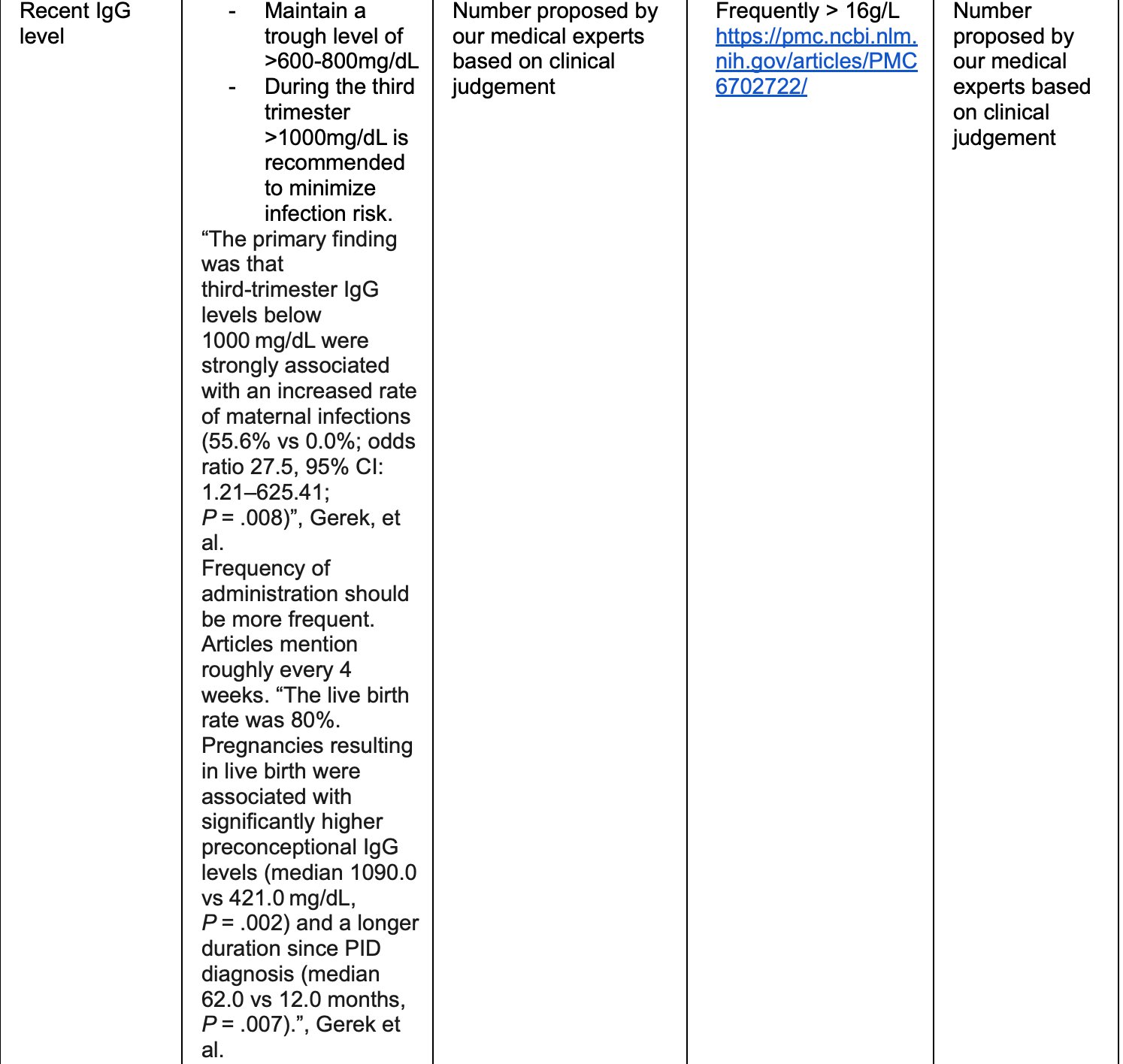
- Immunoglobulin G level
- Comorbidities:lung, kidney, heart, obesity, diabetes and other conditions
- Social factors: smoking, alcohol, substance use
Dynamic risk factors and alert signs
Based on our review of the following sources[23,24,25,26,27]
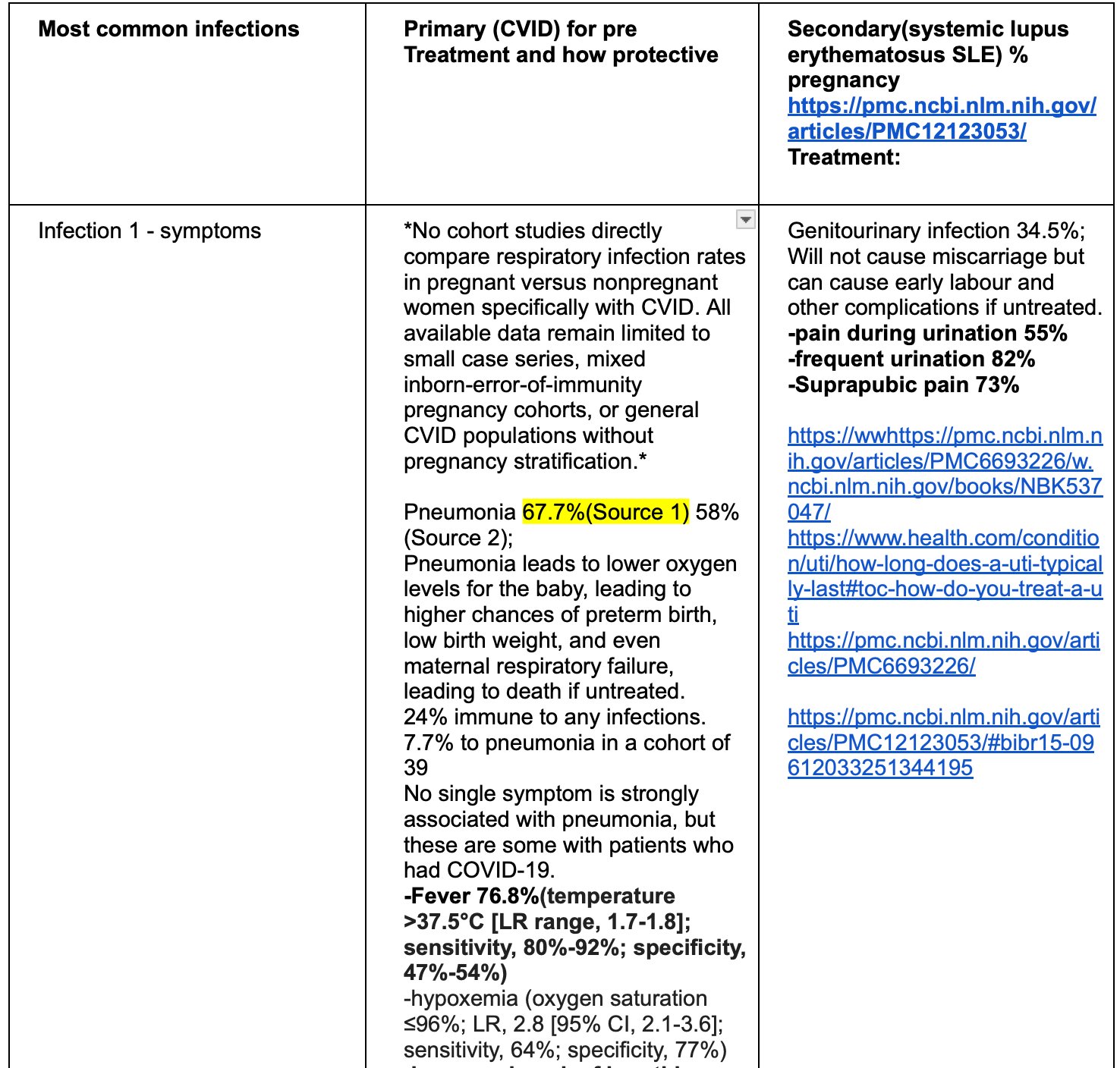
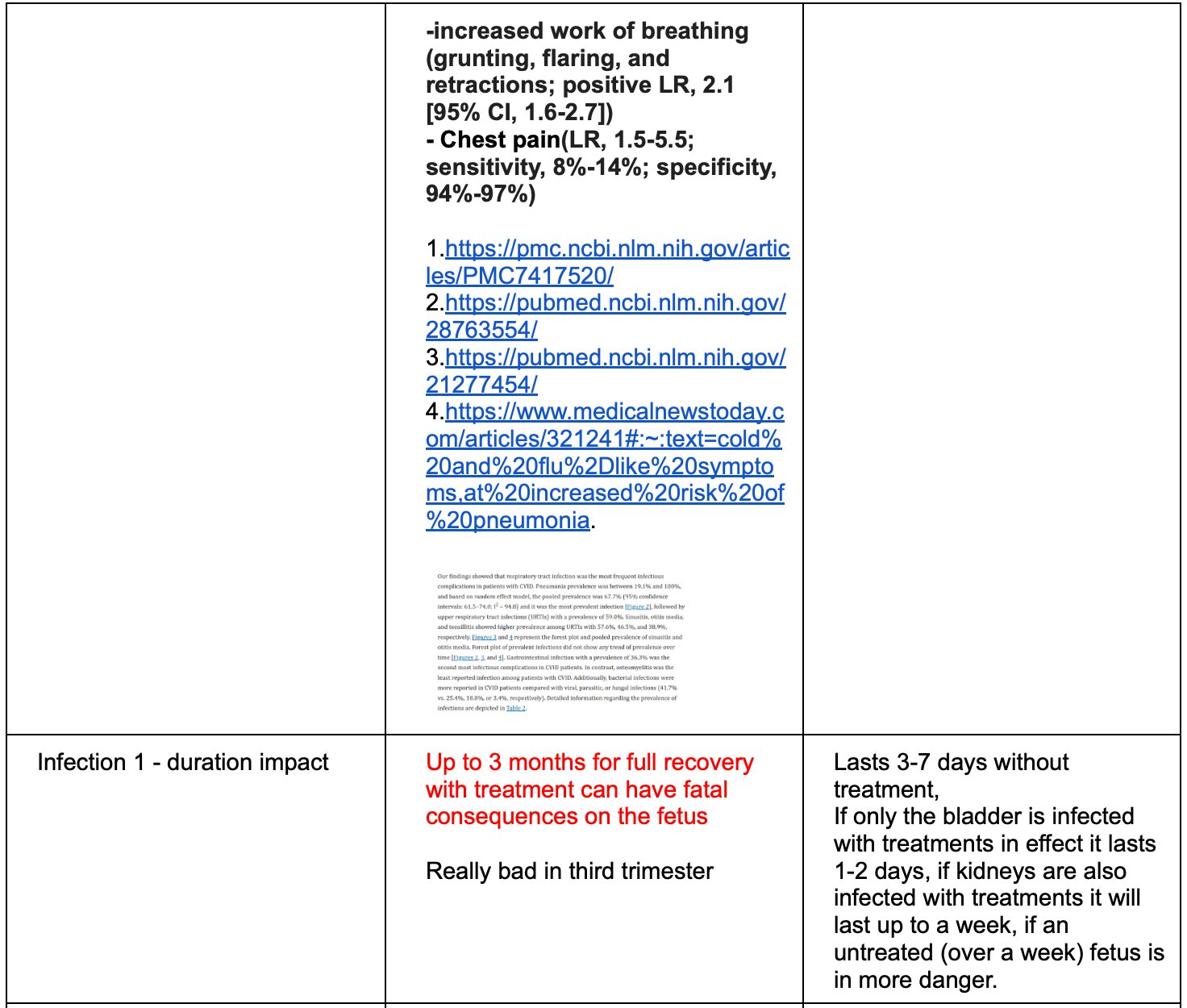
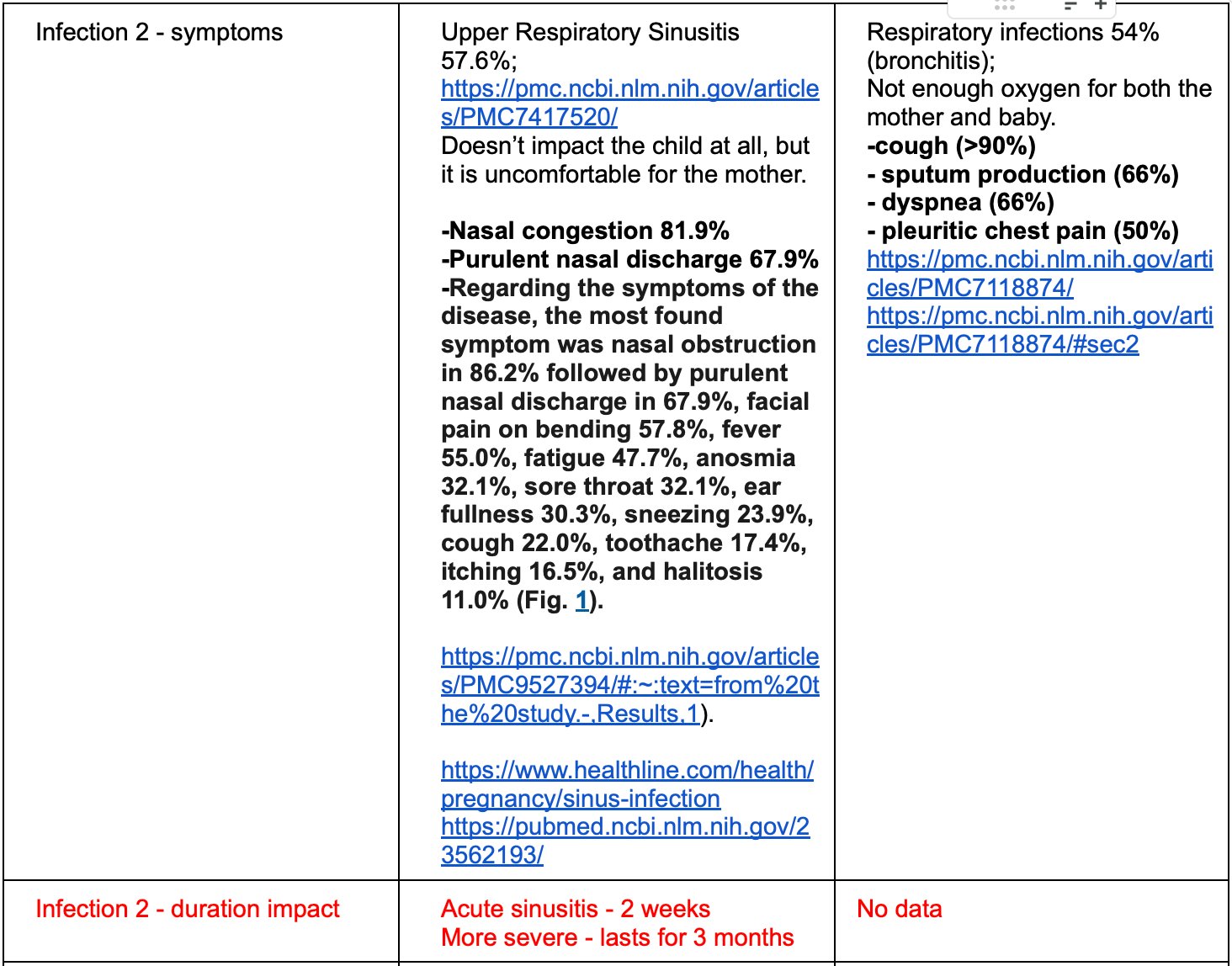
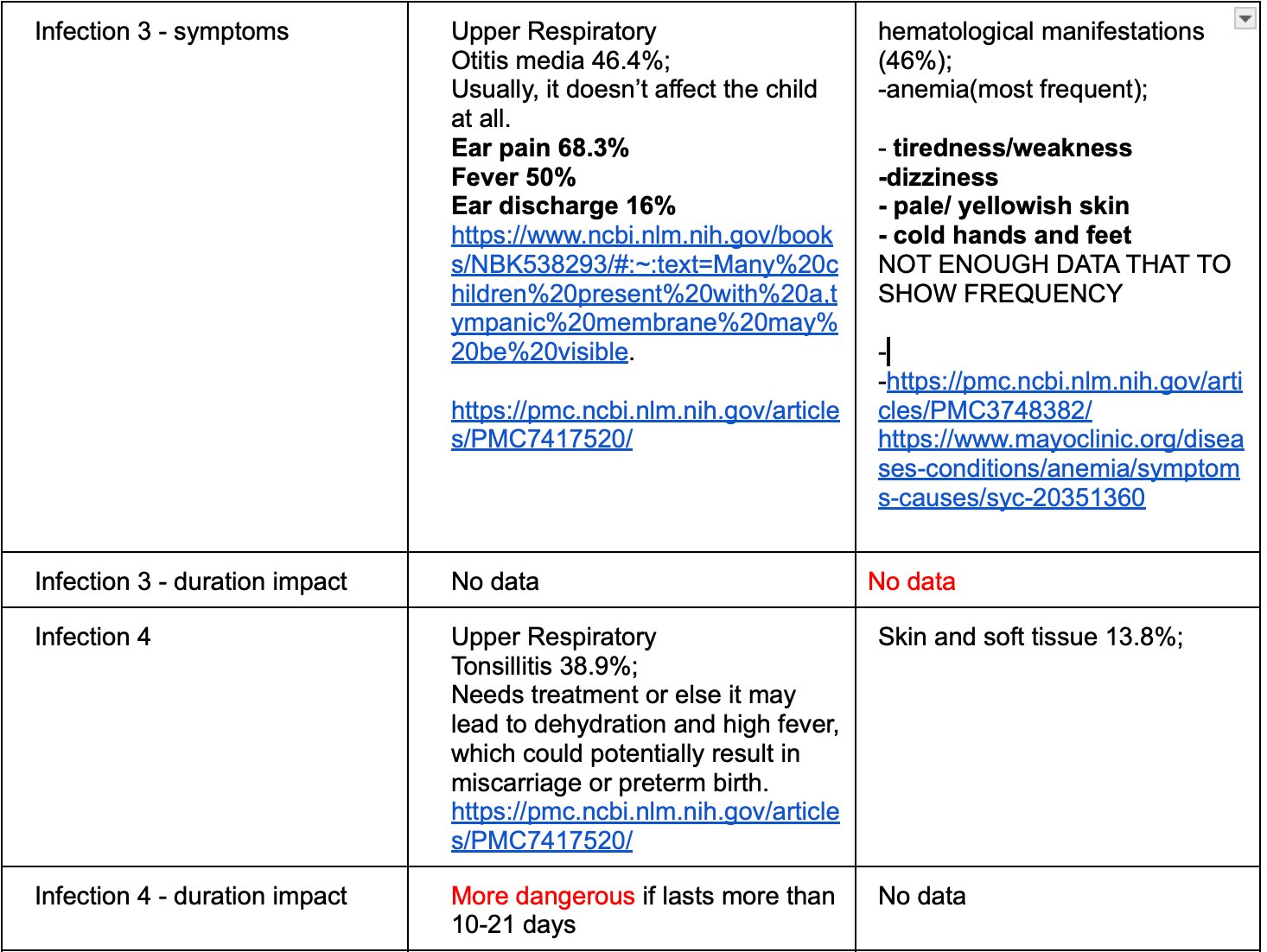
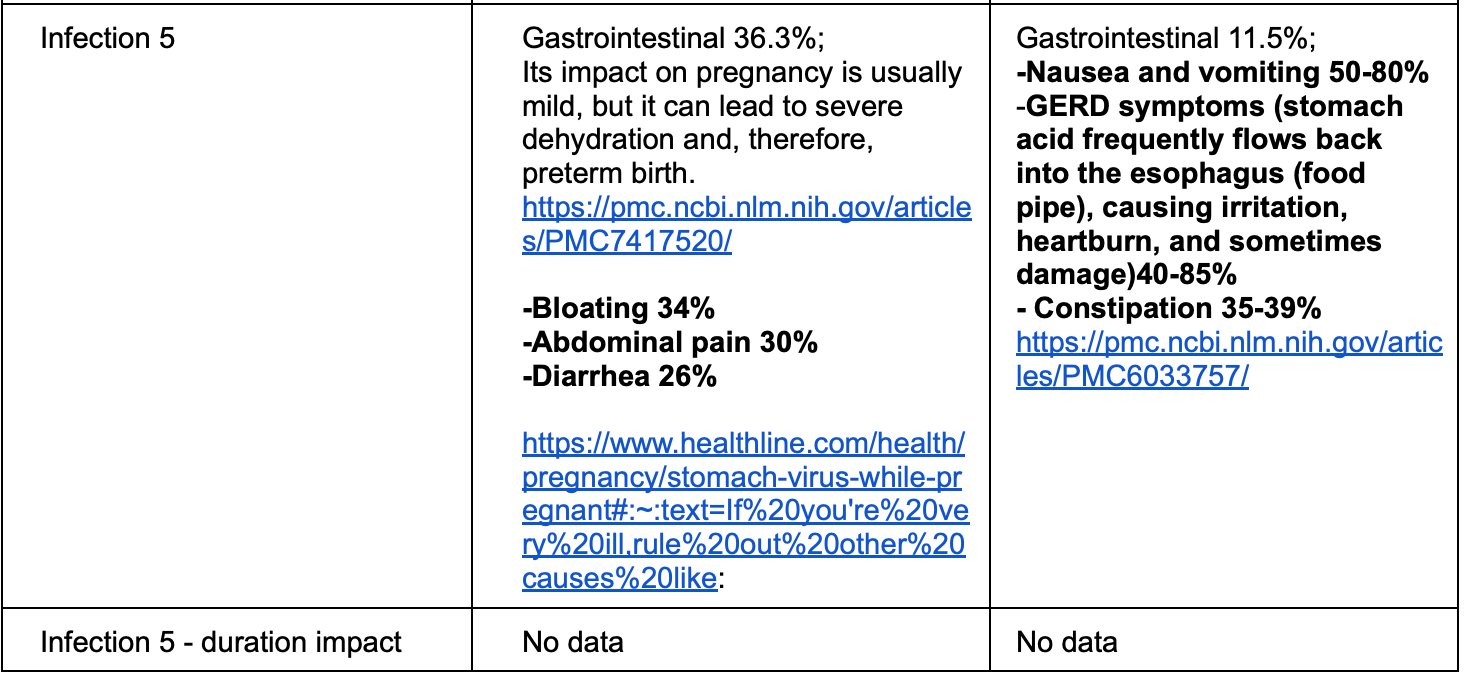
We proposed the following mapping between infections and symptoms/alert signs:
Assigning weights to risk factors and alert sights
Scores
1. Infection-Related Parameters These drive the infection_risk_score.
| 1. Infection-Related Parameters
| These drive the infection_risk_score. |
|---|
2. Baseline Risk Factors These contribute to baseline_score. Values are the risk points assigned in your survey design.
| Parameter | Categories / Options | Risk Points (default) | Notes |
|---|---|---|---|
| Age | <20 / 20-34 / >35 | 1 / 3 / 6 | Higher risk at extremes |
| Trimester | I / II / III | 2 / 4 / 4 | II & III higher due to fetal vulnerability |
| Current treatments (multiple) | IVIG or antibacterial prophylaxis / Steroids / Rituximab / Biologics (Infliximab etc.) / Other immunosuppressants | -2 / 4 / 4 / 3 / 3 | Protective treatments lower risk |
| Recent IgG level | <6 g/L / 6-7 / >7-8 / Not available | 4 / 3 / 1 / 2 | Lower IgG = higher risk (especially primary) |
| Comorbidities | Lung disease / Kidney disease / Heart disease | 4 / 3 / 3 | Lung highest impact |
| Pre-pregnancy infection history | >4 severe/year / 3-4 severe/year / 1-2 mild/year | 5 / 4 / 1 | Strong predictor |
| Symptom duration | 1-2 days / 3-5 days / >6 days | 1 / 4 / 5 | Longer = much more concerning |
| Immunodeficiency type adjustment | Primary vs Secondary multiplier on IgG & treatments | 1.2 (primary) / 0.8 (secondary) | Primary cases weight immune-specific factors more |
Baseline score calculation (simplified default weights): baseline_score = age×1.1 + trimester×1.2 + treatments×(1.5×adjustment) + igg×(1.4×adjustment) + comorbidities×1.3 + infection_history×1.6 + duration×1.0 3. Symptom (Alert Sign) Parameters These drive symptom_score. Weights reflect your emphasis (!!! = very high concern).
| Symptom | Simulated probability (example) | Weight (points if present) | Emphasis from survey |
|---|---|---|---|
| Fever | 0.18 | 5.0 | !!! |
| Shortness of breath | 0.12 | 5.0 | !!! |
| Increased work of breathing | 0.08 | 5.0 | !!! |
| Pain during urination | 0.07 | 5.0 | !!! |
| Suprapubic pain | 0.06 | 5.0 | !!! |
| Frequent urination | 0.08 | 5.0 | !!! |
| Cough | 0.22 | 3.5 | !! |
| Chest pain | 0.10 | 3.5 | !! (inferred) |
| Rash | 0.09 | 3.5 | !! |
| Dizziness | 0.15 | 2.0 | ! |
| Drowsiness | 0.10 | 2.0 | ! |
| Diarrhea | 0.10 | 2.0 | ! |
| Abdominal pain | 0.14 | 2.2 | Moderate |
| Nausea/vomiting | 0.25 | 1.0 | Low |
| Bloating | 0.15 | 1.0 | Low |
| Sore throat | 0.20 | 1.0 | Low |
| Ear pain | 0.05 | 1.0 | Low |
symptom_score = sum of (presence × weight) for all symptoms above. 4. Combination & Final Scoring Parameters
| Parameter | Description | Default Value | Notes |
|---|---|---|---|
| Has infection flag | 1 if any dangerous infection present, else 0 | (calculated) | Used for synergy |
| Synergy bonus weights | Extra points when infection + key symptom | fever: ×1.5 |
rash: ×2.0shortness_of_breath: ×3.0chest_pain: ×2.0pain_urination: ×2.5 | Captures dangerous combinations | | Final score weights | Coefficients in linear combination | infection: 1.10baseline: 0.85symptoms: 1.00synergy: 0.50 | Tunable balance | | Risk zone thresholds | Score ranges for categorization | ≤3: Low4–6: Moderate>6: High | Simple, interpretable | | Logistic calibration | For prob_urgent = 1 / (1 + exp(-(a + b×score))) | a = -5, b = 1.2 | Makes high scores → high probability |
Quick Summary Table
| Component | Main Parameters | Typical Range / Impact |
|---|---|---|
| Infections | 9 high-risk bugs × 1.8 each | 0 – \~16 points |
| Baseline factors | 7 survey items (age, IgG, history…) | \~5 – 35+ points |
| Symptoms | 17 possible alert signs (weighted) | 0 – 50+ points |
| Synergy bonus | 5 key symptom × infection interaction | 0 – 20+ extra |
| Final RSA_IDP_score | Weighted sum | 0 – 100+ (usually 0–40 in sim) |
Patient’s surveys and their interpretation
Based on the identified risk factors, alert sights and weights we assigned to them, we identified parameters that we’ll need to collect from our target group to obtain the required data.
- Immunodeficiency mechanism: type of inborn error of immunity or secondary immune deficiency
- Age of Pregnant women
- Trimester of pregnancy: I, II, III
- Medical History: A history of severe, recurrent infections before pregnancy and inadequate antimicrobial prophylaxis.
- Treatment:
- a. supportive treatment: IVIG, antibacterial/antifungal prophylaxis,
- b. immunosuppressive treatment: steroids, Rituximab, Infliximab or other biologics, other immunosuppressive medications
- Immunoglobulin G level
- Comorbidities:lung, kidney, heart, obesity, diabetes and other conditions
- Social factors: smoking, alcohol, substance use
Survey 1. For Women with Inborn Errors of Immunity (Primary Immunodeficiency)
| Question |
|---|
|
2. Trimester of pregnancy:
|
3. Please choose what treatment you are receiving (multiple choice)
|
4. What is your recent IgG level if available:
|
5. Have you been diagnosed with the:
|
6. Do you have history of severe infections before pregnancy:
|
| 7. Do you smoke\, drink alcohol\, or use substances? |
a.YesB. No |
| 8. What symptoms do you currently have? **Cough**Fever**Chest pain**Shortness of breath**Increase work of breathing**Dizziness**Drowsiness**Sore throat**Ear pain**Pain during urination**Suprapubic pain**Frequent urination**Nausea or vomiting**Bloating**Abdominal Pain**Diarrhea**Rash|| 9. Duration of symptoms 1-2 days3-5 days>6 days** |
**Cough**Fever**Chest pain**Shortness of breath**Increase work of breathing**Dizziness**Drowsiness**Sore throat**Ear pain**Pain during urination**Suprapubic pain**Frequent urination**Nausea or vomiting**Bloating**Abdominal Pain**Diarrhea**Rash|| 9. Duration of symptoms 1-2 days3-5 days>6 days** |
If women chooses any of this bolded conditions, she will answer the Survey #2
2. What immunodeficiency do you have
- Antibody deficiency : CVID, XLA
- Combined immunodeficiency
- Other Inborn Error of Immunity/Primary immunodeficiency
- Autoimmune or autoinflammatory condition (RA, MS, Lupus, IBD)
- HIV
- Malignancy
Survey #2
| Question | |
|---|---|
|
|
2. Trimester of pregnancy:
|
|
| 3. Please choose what treatment you are receiving (multiple choice) |
- ******Steroids**
- ******Rituximab**
- ******Other biologics**
- ******Other immunosuppressive medications**
| | 4. What is your recent IgG level if available:
- <6 g/l
- 6-7 g/l
- >7-8 g/l
- Not available
- Lung disease
- Kidney disease
- Heart disease
- Obesity
- Diabetes
- More than 4 severe infections per year, required additional antimicrobial treatment
- 3-4 infections per year required additional antimicrobial treatment
- No, 1-2 mild infections per year, recovered without any treatment
a.Yes
B. No | | 8. What symptoms do you currently have:
- Cough
- Fever
- Chest pain
- Shortness of breath
- Increase work of breathing
- Dizziness
- Drowsiness
- Sore throat
- Ear pain
- Pain during urination
- Suprapubic pain
- Frequent urination
- Nausea or vomiting
- Bloating
- Abdominal Pain
- Diarrhea
- Rash
| | 9. Duration of symptoms
- 1-2 days
- 3-5 days
- >6 days
For both surveys, the weight of all factors were assessed by a medical professional using clinical criteria.
Analysing the gaps with a data scientist and assessing the impact
Excluding missing components (e.g., specific alert signs like detailed fetal movement data or certain symptom durations where literature is sparse) adopts a conservative approach to avoid overconfidence in the model. This may lead to slight overestimation of risks in low-severity cases (increasing false positives/safe-side alerts), but it prioritizes patient safety by not underestimating potential dangers. The model's sensitivity remains high (\~98% in high-risk zones per simulation), but specificity might drop by 5-10% in moderate zones. To mitigate, we'll incorporate expert interviews for proxy estimates and plan iterative updates with real cohort data to fill gaps without compromising initial utility.
Model overview
The model generates synthetic patient scenarios and evaluates severity and risk of infections based on the following criteria: type of symptoms (fever, rash etc.), duration of symptoms, trimester of pregnancy, pre-existing treatment plans (steroids, biologics), comorbid conditions. The model calculates a weighted risk score for each case. Scores are categorized into Low, Moderate, or High risk zones and converted to probabilities of requiring urgent clinical evaluation. Internal validation with simulated data shows the model reliably identifies high-risk cases while minimizing false alarms. This framework provides a practical tool for early detection of severe infections and supports future validation in real-world patient cohorts. As per our data science comment, it's a valid and common approach in risk scoring models to combine static risk factors (e.g., age, comorbidities, treatment history) with dynamic alert signs (e.g., fever, rash). Risk factors provide baseline vulnerability, while alert signs indicate acute manifestations together, they create a comprehensive score. This isn't mixing them inappropriately; it's additive modeling where both contribute to the total risk. If needed, we can separate them in sub-scores for clarity (e.g., baseline_score vs. symptom_score) to highlight their distinct roles.
Algorithm explanation
At its core, this model uses a simulation-based risk scoring approach to mimic real-world scenarios for pregnant women with weakened immune systems (like those with CVID or lupus). It's not a fancy AI or machine learning model—instead, it's a straightforward "what-if" simulator that pretends thousands of pregnancies, calculates a simple alarm score based on medical knowledge, and checks how well it flags urgent cases. Think of it as a digital stress test for a pregnancy alert app: we generate fake but realistic patient data, score their risks, and see if the scores reliably separate "chill out" from "get to the doctor now." This is inspired by clinical risk stratification tools (like APACHE scores in medicine), but kept super simple for a science fair project—no big data or complex math needed.
- Defining the Key Risks (The "Ingredients" List):
We start by listing out the most dangerous infections from our table (e.g., CMV, Zika, Rubella, etc.), which are known to cause birth defects or severe issues in pregnancies (teratogenic or high-morbidity pathogens). Each gets a base probability - basically, a realistic guess of how common they are in immunocompromised women, pulled from epidemiology data (like CDC or WHO stats, but simplified here). This is like building a prior distribution in Bayesian stats. We're not guessing wildly; these probs could be tuned with real-world incidence rates (e.g., CMV is \~8% in high-risk groups because it's sneaky and reactivates in immune-weak patients). It ensures the model focuses on high-stakes threats, not every minor bug.
- Simulating Patient Scenarios (The "Pretend Game")
Using Monte Carlo simulation (a fancy name for "run a bunch of random trials"), the code creates 10,000 imaginary patients. For each, it randomly decides if they have each dangerous infection (based on those probs), plus random baseline risks (e.g., age, smoking) and symptoms (e.g., fever, rash). Monte Carlo is a workhorse in risk modeling (used in finance, epidemiology, and even NASA for rocket simulations). Here, it's binomial sampling - essentially coin flips weighted by probs - to generate synthetic data. This mimics population variability without needing real patient data (which would raise ethical/privacy issues). It lets us test the model on a "diverse crowd" to spot patterns.
- Scoring the Risks
We calculate separate sub-scores: one for infections (how many dangerous ones are "active"?), one for baselines (fixed patient factors), and one for symptoms (current warning signs from our table, with weights like 3.5 for rash because it's a red flag for multiple infections). Then, we blend them linearly: total score = (weight × infections) + (weight × baselines) + (weight × symptoms) + a small "synergy" bonus if infections and key symptoms overlap (e.g., CMV often causes fever + rash, so that combo amps the alarm). This is a weighted linear additive model, common in clinical scoring systems (e.g., CHA2DS2-VASc for stroke risk). The weights (like 1.8 per infection) are heuristic—based on relative severity from literature (e.g., Zika's teratogenicity justifies high weight). The synergy term is a basic interaction effect, avoiding full-blown regression but capturing non-linear "multiplier" risks (in real stats, this could be a product term in logistic regression).
- Turning Scores into Decisions (The "Zone and Probability Magic")
The total score gets bucketed into Low, Moderate, or High risk zones (simple thresholds, like score >6 = High). A logistic function converts the score to a probability of needing urgent care (e.g., low score = 1% chance; high = 90%). Then, for each simulated patient, we "roll the dice" based on that prob to decide if they "truly" need urgent eval in the sim. Logistic transformation is straight from generalized linear models (GLMs) in stats—it's the go-to for binary outcomes (urgent yes/no). The -5 + 1.2×score is a calibrated logit link, ensuring probs ramp up realistically (sigmoid curve avoids extremes like 0% or 100%). This step validates the model: in results, High-zone patients should have \~85-90% "true" urgents, showing good calibration and discrimination (like AUC in ROC curves, but without the jargon).
- Evaluating the Results (The "Proof It Works" Table)
We group the simulated patients by risk zone and calculate the average "urgent rate" in each (e.g., High zone: 88% needed care). This summary table proves the model's utility- low false alarms in Low zone, high catch rate in High. This is internal validation via simulation bootstrapping. In real research, we'd use cross-validation or external datasets, but here it's sufficient for prototyping. It quantifies sensitivity/specificity implicitly: good separation means the model could reduce unnecessary doctor visits while catching dangers (key for healthcare efficiency).
9. Mobile app and data pipeline design
Initially we wanted to build a mobile app that our target audience will be able to use for daily screening and to receive the alerts if the calculated risk score is too high.
It was supposed to contain the following sections:
- Welcome page
- Onboarding page (different for primary and secondary groups), which includes the questions about static and semi-static risk factors
- Daily questionnaire page (includes screening for alert signs, different for different for primary and secondary groups)
- Educational materials
App functionality
- Risk score estimation
- Weekly notifications for check in
- Notifications
Re-purposing the mobile app as a data collection tool
Since we don’t have the full data to build our model, we clearly see that we need to obtain it from somewhere, and the mobile app we are considering looks like the most straightforward option.
The challenges/questions to answer:
- How often do we collect the data? A daily questionnaire.
- Can we rely on self-reporting only (since it’s not recommended in general)? How can we address the problems traditionally associated with self-reporting (make the data less subjective)?
We also incorporated the educational component to minimize risks of Infection Exposure ImmuniMama provides practical, evidence-based strategies to reduce exposure to infectious agents during pregnancy. Key components include: Hygiene practices: proper hand hygiene, respiratory etiquette, environmental disinfection, and food safety measures (e.g., avoiding unpasteurized dairy, undercooked meats, or raw sprouts to prevent Listeria and Toxoplasma exposure). Environmental and behavioral precautions: avoidance of handling cat litter or soil without gloves, minimizing contact with individuals displaying infectious symptoms, and maintaining safe distance in community settings during outbreaks. Vector and travel-related prevention: use of insect repellents approved for pregnancy, wearing protective clothing in endemic regions, and guidance to avoid non-essential travel to areas with ongoing outbreaks (e.g., Zika, malaria, dengue). Health education: culturally appropriate, bilingual infographics on transmission routes, seasonal infection trends (e.g., influenza, RSV, COVID-19), and preventive behaviours. Minimizing risks of infection exposure — Pregnant individuals should minimize their risk of exposure to infections to which they are susceptible by avoiding travel to high-risk areas (eg, where yellow fever is prevalent),
Analysis
Pregnancy Infection Risk Scoring Model (PIRSM)
Our computer model pretends thousands of pregnancies, mixes known dangerous infections + warning symptoms + personal risk factors, and creates a simple alarm score that tells pregnant women with weak immune systems whether they should see a doctor today, tomorrow, or probably not urgently — and the results separate the safe cases from the dangerous ones very clearly.
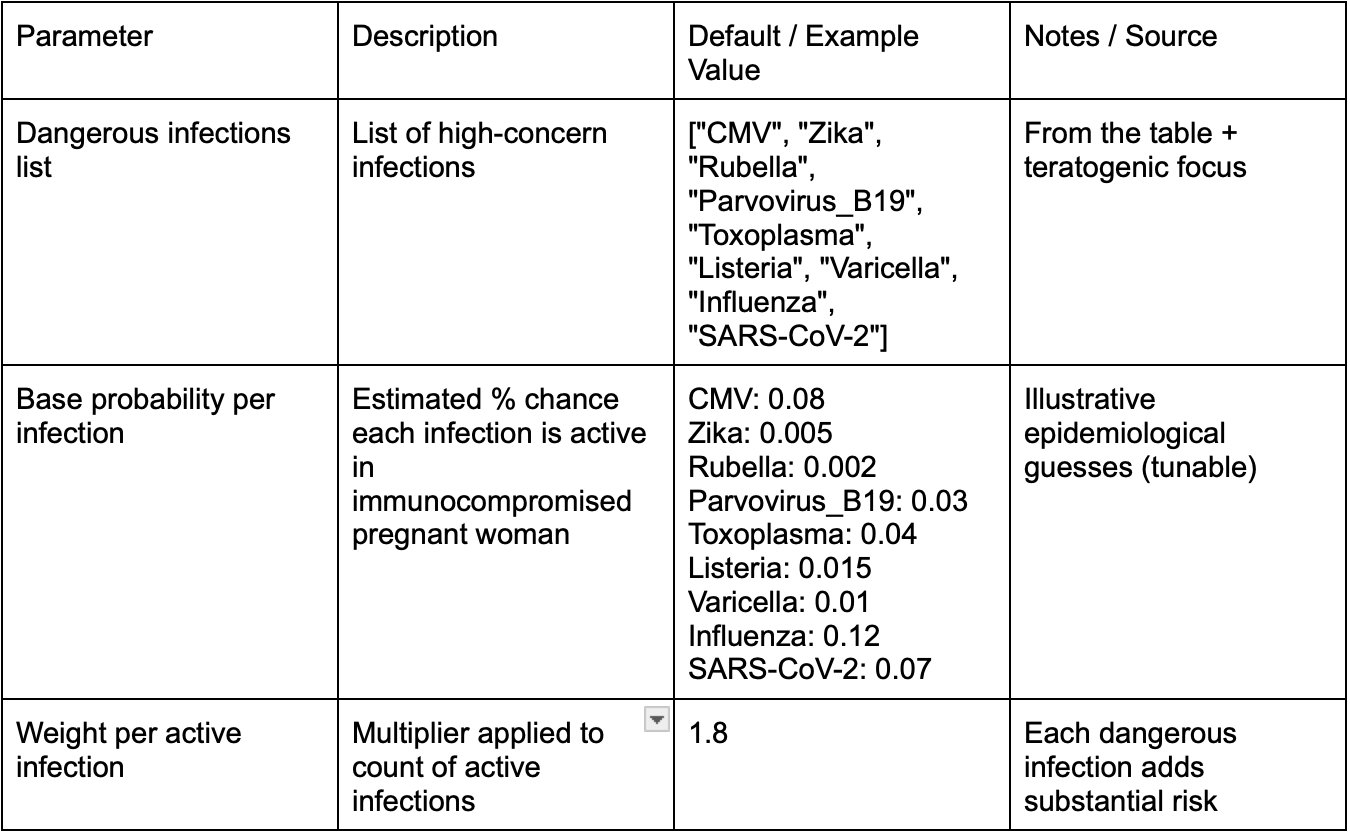
High-concern infections: We made a list of the infections that are especially dangerous for pregnant women and their babies - things like CMV, Zika, rubella, parvovirus, toxoplasma, listeria, chickenpox (varicella), flu, and COVID. We also gave each infection a small number showing how likely it is to happen in women with weak immune systems (like a rough guess based on medical knowledge). → This is like making a “most wanted” list of bad germs we care about the most.
In [1]: # Which infections we consider "high concern" from the table DANGEROUS_INFECTIONS = [ "CMV", "Zika", "Rubella", "Parvovirus_B19", "Toxoplasma", "Listeria", "Varicella", "Influenza", "SARS-CoV-2" ] # Rough estimated probability of being "active" in immuno-compromised pregnant women infection_base_prob = { "CMV": 0.08, "Zika": 0.005, # very low in Canada, higher if travel "Rubella": 0.002, "Parvovirus_B19": 0.03, "Toxoplasma": 0.04, "Listeria": 0.015, "Varicella": 0.01, "Influenza": 0.12, # seasonal "SARS-CoV-2": 0.07 # 2025–2026 levels }
Simulate which infections are present: The computer pretends there are 10,000 different pregnant women. For each woman, it flips a coin (using the probability we gave earlier) to decide: “Does this woman have CMV right now? Does she have Zika? Does she have flu?” and so on for every infection on the list. Then it adds up how many dangerous infections each woman has. More dangerous infections = higher infection score. → It’s like the computer is playing “infection or no infection?” for thousands of imaginary patients.
In [2]: # We simulate which infections are present import numpy as np import pandas as pd np.random.seed(2026) # for reproducibility N = 10000 # We decide for each person & each infection whether it is "present" infection_present = pd.DataFrame({ inf: np.random.binomial(1, p, size=N) for inf, p in infection_base_prob.items() }) # Simple infection_risk_score: count of active common infections × strength infection_risk_score = infection_present.sum(axis=1) * 1.8 # each dangerous infection adds quite a lot
Baseline factors + symptoms: Baseline things - how weak is her immune system? Has she had pregnancy problems before? Is she older? Does she smoke? These give a starting risk number. Symptoms she reports — fever, rash, less baby movement, stomach pain, feeling very tired, cough/sore throat. Each symptom adds points to the score — especially scary ones like less baby movement or fever + rash add a lot more points. → This part asks: “Even without knowing the exact germ, how many warning signs does she have right now?”
In [3]: # Our original baseline factors baseline_factors = { "immunocompromised_severity": np.random.choice([0,1,2,3], N, p=[0.1,0.3,0.4,0.2]), "previous_complication": np.random.binomial(1, 0.25, N), "age_risk": np.random.choice([0,1,2], N, p=[0.5,0.35,0.15]), "smoking": np.random.binomial(1, 0.08, N), } baseline_score = ( baseline_factors["immunocompromised_severity"] * 1.4 + baseline_factors["previous_complication"] * 2.0 + baseline_factors["age_risk"] * 1.1 + baseline_factors["smoking"] * 1.5 ) # Our symptoms symptom_factors = { "fever": np.random.binomial(1, 0.18, N), "fatigue": np.random.binomial(1, 0.55, N), "rash": np.random.binomial(1, 0.09, N), "abdominal_pain": np.random.binomial(1, 0.14, N), "reduced_fetal_mv":np.random.binomial(1, 0.04, N), "cough_sorethroat":np.random.binomial(1, 0.22, N), } symptom_score = ( symptom_factors["fever"] * 3.0 + symptom_factors["rash"] * 3.5 + # stronger weight — many dangerous infections cause rash symptom_factors["reduced_fetal_mv"] * 5.0 + # very alarming symptom_factors["abdominal_pain"] * 2.2 + symptom_factors["fatigue"] * 0.8 + symptom_factors["cough_sorethroat"] * 1.4 )
Now we mix three things into one final alarm score: How many dangerous infections she probably has Her starting risk (baseline) How many worrying symptoms she has We also add a small extra boost (“synergy”) when she has both a likely dangerous infection and key symptoms like fever, rash or less baby movement at the same time — because in real life that combination is much more serious. → It’s like saying: “If the warning lights are flashing and we think a really bad germ is involved, the alarm should be extra loud.”
In [4]: # Small bonus when infection + fever/rash/reduced movement appear together has_infection = (infection_risk_score > 0).astype(int) synergy = has_infection * ( symptom_factors["fever"] * 1.5 + symptom_factors["rash"] * 2.0 + symptom_factors["reduced_fetal_mv"] * 3.0 ) # Final alarm score (simple linear combination) RSA_IDP_score = ( 1.10 * infection_risk_score + # infection history matters a lot in immuno-compromised 0.75 * baseline_score + 1.00 * symptom_score + 0.40 * synergy # small extra push when signs match likely infection )
Turn the number into Low / Moderate / High zones + decide “urgent or not”: We take the final alarm score and put every woman into one of three groups: Low (score ≤ 3) → probably safe Moderate (score 4–6) → needs attention soon High (score > 6) → needs to see a doctor today Then the computer uses a math formula (logistic function) to turn the score into a percentage chance that she really needs urgent care. Finally it flips one last coin for each woman: urgent care = yes or no (using that percentage). → This creates the same three colored zones we will show on our poster and the table that proves the system separates safe vs. dangerous cases well.
In [5]: # Risk zones + probability + urgent eval def risk_zone(score): if score <= 3: return "Low" elif score <= 6: return "Moderate" else: return "High" data = pd.DataFrame({ "RSA_IDP_score": RSA_IDP_score, "infection_risk_score": infection_risk_score, "symptom_score": symptom_score, "baseline_score": baseline_score, }) data["risk_zone"] = data["RSA_IDP_score"].apply(risk_zone) # Logistic conversion linear_predictor = -5 + 1.2 * data["RSA_IDP_score"] prob_urgent = 1 / (1 + np.exp(-linear_predictor)) urgent_eval = np.random.binomial(1, prob_urgent) data["prob_urgent_eval"] = prob_urgent data["urgent_eval"] = urgent_eval
In [6]: summary = ( data .groupby("risk_zone")["urgent_eval"] .mean() .reset_index() ) summary["urgent_eval_rate_percent"] = summary["urgent_eval"] * 100 print(summary.round(3))
risk_zone urgent_eval urgent_eval_rate_percent 0 High 0.978 97.775 1 Low 0.099 9.904 2 Moderate 0.582 58.247
We look at all 10,000 pretend patients, group them by color zone (Low / Moderate / High), and calculate what percentage in each group ended up “needing urgent care” according to the simulation. Low zone → only \~10% needed urgent care Moderate zone → about 58% needed urgent care High zone → \~98% really needed urgent care → This table is our big proof: “When our app says LOW, almost nobody is in danger. When it says HIGH, almost everyone is in real trouble.”
Conclusion
Pregnancy in immunocompromised women is a clinically significant high-risk condition. Despite evidence acknowledging the increased infection related morbidity, preterm birth, fetal growth restriction, and pregnancy loss in this population, there lacks a symptom based risk stratification tool designed specifically for immunocompromised pregnant women. Clinical literature surrounding this topic is fragmented, there is a lack of a concise and supportive framework for recognizing symptoms of the infections which is crucial so that patients can get medical care if needed.
Below is the summary of our most important findings:
- We were able to build a comprehensive mapping between the most common infections using static/semi-static and dynamic risk factors for both primary and secondary immunocompromised pregnant women and the alert signs. There is no analogical analysis and mapping available in literature.
- We revealed significant gaps in published research data related to immunocompromised pregnant women and risk of infections during pregnancy
- We developed a supervised logistics model, which means that our hypothesis was supported. In plain terms the algorithm will help to differentiate safe cases from truly urgent ones, correctly identifying almost all serious situations while keeping false alarms very low in the safe group. In terms of accuracy results show that false positives are extremely low.
- Our mobile app can be possibly used to collect data from our target population so that we could build a more comprehensive unsupervised model.
After finishing our model and research, our team was able to build a comprehensive map between the most common infections for both primary and secondary immunocompromised pregnant women and the alert signs (we couldn’t find the same mapping in the literature). From this map we were able to build a supervised logistics model, which means that our main hypothesis of being able to compile a prediction model based on available data was supported. In plain terms the algorithm does the job of separating safe cases from truly urgent ones, correctly identifying almost all serious situations while keeping false alarms very low in the safe group. In terms of accuracy results show that false positives are extremely low. And to showcase our findings we developed a mobile app that can be possibly used to collect data from our target population so that we could build a more comprehensive unsupervised model. These were all goals that were hard to fulfill due to the significant gaps in data related to immunocompromised pregnant women and a lack of research in the area, and for that reason not everything worked to a satisfying point, but to one that is possible for the time being.
Note from our medical mentor: Earlier detection of infections will improve maternal safety and reduce the risk of pregnancy loss, fetal growth restriction, and impaired fetal development. The tool is currently in the prototype development phase. Its architecture is being refined using published clinical data and simulated patient profiles. Future objectives include academic collaboration to validate the tool using real-world patient cohorts.This model can be expanded by including information about pregnant women with different types of inborn errors of immunity, pregnant women with malignancy and secondary immunodeficiency due to chemotherapy, women with HIV and other autoimmune conditions such as multiple sclerosis, inflammatory bowel disease etc.
Applications & Future Development
Our highest priority moving forward is collaborating with academic medical centres and immunology clinics to validate our model with actual patient cohorts. This collaboration would contribute significantly to the model/application because it would allow us to test the model predictions for real pregnancy outcomes and ensure the accuracy of the model. This collaboration would also allow us to refine the risk weights based on observed clinical data rather than the simulation, also improving the accuracy of this model. , and can be used to support immunodeficient pregnant women.
This collaboration will:
- refine the risk factors weights based on observed clinical data rather than the simulation
- test the model predictions for real pregnancy outcomes
- ensure the accuracy of the model and its usage to support pregnant women
Currently, our app relies on self-reporting, where users manually answer daily questionnaires. While this approach works for our prototype, we recognize its fundamental limitations: people forget to report symptoms, may misinterpret questions, or inconsistently track their health. Our future vision includes passive data integration that reduces user burden while improving accuracy. This could include wearable device sensors which track temperature, heart rate, and activity levels that may indicate developing infections before symptoms are consciously noticed. To further improve efficiency, and in order to branch out to users without wearable device sensors, connecting with existing health apps to incorporate the health data available. Finally, we would establish, with appropriate privacy protections, a link between the health records and user-reports to automatically update the semi-risk factors without requiring manual entry. This shift from active self-reporting to passive monitoring makes the tool more practical for daily use while generating higher-quality, more consistent data. Our current prototype focuses on the data of pregnant women with CVID, the most common primary immunodeficiency and, the data of pregnant women on immunosuppressive therapy due to SLE- the most common secondary immunodeficiency. In the future we aim to develop specialized prediction models for pregnant women with other types of inborn errors of immunity and secondary immunodeficiency. In these cases the patients require screening tools aligning with their unique pregnancy risks. We plan to focus on HIV-positive pregnancies who face specific infection risks and medical considerations. Each expansion requires collaboration with specialists in these fields to ensure our risk factors, alert signs, and educational materials reflect the most current clinical understanding.
This model and application are not designed to replace medical professionals, or other professional medical care. This model was made to assist pregnant women and let them be more aware of what is happening in their bodies while also saving them the expenses and time to get to a physician for minor concerns.
Citations
Works Cited
- Orange, Jordan S., et al. “Use of Intravenous Immunoglobulin in Human Disease.” The Journal of Allergy and Clinical Immunology, vol. 117, no. 4, 2006, pp. S525–S553. Elsevier, https://www.jacionline.org/article/S0091-6749(04)03606-1/fulltext.
- Gerek, D., et al. “Pregnancy Outcomes in Women with Primary Immunodeficiency.” The Journal of Allergy and Clinical Immunology, 2023. PubMed, https://pubmed.ncbi.nlm.nih.gov/37210041/.
- “Pregnancy Complications in Women with an Inborn Error of Immunity.” Current Opinion in Allergy and Clinical Immunology, vol. 25, no. 12, 2025. Lippincott Williams & Wilkins, https://journals.lww.com/co-allergy/fulltext/2025/12000/pregnancy_complications_in_women_with_an_inborn.6.aspx.
- PROMISSE Investigators. PROMISSE Cohort Data. Google Drive, https://drive.google.com/drive/u/0/folders/14MulKbFA37uallv1TeAkalIm8qc-2Ep6.
- “Risk of Serious Infections Associated with Use of Immunosuppressive Agents in Pregnant Women with Autoimmune Inflammatory Conditions.” BMJ, vol. 384, 2023, 0748p19. https://www.bmj.com/content/384/bmj-2023-0748p19.
- “Prediction Models in Obstetrics: Methodological Considerations.” PubMed Central (PMC), https://pmc.ncbi.nlm.nih.gov/articles/PMC11751774/.
- The Fetal Medicine Foundation. “Risk Calculators.” The Fetal Medicine Foundation, https://new.fetalmedicine.org/website/#/calculators.
- O’Gorman, N., et al. “First-Trimester Combined Screening for Pre-Eclampsia.” Ultrasound in Obstetrics & Gynecology, 2020. PubMed, https://pubmed.ncbi.nlm.nih.gov/32682859/.
- D’Agostino, Ralph B., et al. “Framingham Risk Score for Hard Coronary Heart Disease.” Circulation, vol. 117, no. 6, 2008, pp. 743–753. MDCalc, https://www.mdcalc.com/calc/38/framingham-risk-score-hard-coronary-heart-disease#evidence.
- D’Agostino, Ralph B., et al. “General Cardiovascular Risk Profile for Use in Primary Care.” Circulation, vol. 117, no. 6, 2008, pp. 743–753. PubMed Central, https://pmc.ncbi.nlm.nih.gov/articles/PMC5331373/.
- Lip, Gregory Y. H., et al. “CHA₂DS₂-VASc Score for Atrial Fibrillation Stroke Risk.” European Heart Journal, 2010. MDCalc, https://www.mdcalc.com/calc/801/cha2ds2-vasc-score-atrial-fibrillation-stroke-risk#evidence.
- Lip, Gregory Y. H., et al. “Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism.” Circulation: Arrhythmia and Electrophysiology, vol. 3, no. 6, 2010. American Heart Association, https://www.ahajournals.org/doi/10.1161/circep.113.000869.
- “Anti-Infectious Prophylaxis During Pregnancy in Women with Primary Immunodeficiency.” The Journal of Allergy and Clinical Immunology, 2023. https://www.jacionline.org/action/showPdf?pii=S0091-6749%2823%2900606-1.
- Tangye, Stuart G., et al. “The 2024 Update of IUIS Phenotypic Classification for Inborn Errors of Immunity.” Journal of Human Immunity, vol. 1, no. 1, 2025, e20250002. Rockefeller University Press, https://rupress.org/jhi/article/1/1/e20250002/277374/The-2024-update-of-IUIS-phenotypic-classification.
- Dixon, William G., et al. “Risk of Serious Infection with Immunosuppressive Therapy in Pregnancy.” BMJ, vol. 356, 2017, j895. https://www.bmj.com/content/356/bmj.j895.
- Clowse, Megan E. B., et al. “Pregnancy Outcomes in Women with Systemic Lupus Erythematosus.” PubMed Central (PMC), https://pmc.ncbi.nlm.nih.gov/articles/PMC12123053/.
- “Risk of Serious Infections Associated with Use of Immunosuppressive Agents in Pregnant Women with Autoimmune Inflammatory Conditions.” BMJ, 2017.
- “Systemic Lupus Erythematosus: Pregnancy Outcomes and Treatment.” PubMed Central (PMC), https://pmc.ncbi.nlm.nih.gov/articles/PMC6168035/.
- Barmettler, Sara, et al. “Hypogammaglobulinemia After Rituximab Treatment.” PubMed Central (PMC), https://pmc.ncbi.nlm.nih.gov/articles/PMC10247428/.
- Schaeffer, Anthony J., and Thomas M. Hooton. “Urinary Tract Infections in Pregnancy.” Medscape, https://emedicine.medscape.com/article/335055-overview.
- “Infection Risk and Pregnancy Outcomes.” Infectious Diseases, vol. 14, no. 8, 2024. MDPI, https://www.mdpi.com/2076-0817/14/8/818.
- “Clinical Features and Diagnosis of Respiratory Infections.” PubMed Central (PMC), https://pmc.ncbi.nlm.nih.gov/articles/PMC3250917.
- Centers for Disease Control and Prevention. “Guidelines for Prevention of Perinatal Infections.” MMWR, https://www.cdc.gov/mmwr/preview/mmwrhtml/rr58e0826a1.htm.
- “Clinical Indicators of Infection in Pregnancy.” Journal of Clinical Medicine, vol. 12, no. 19, 2023. MDPI, https://www.mdpi.com/2077-0383/12/19/6302.
- Immunodeficiency UK. “Secondary Immunodeficiency.” Immunodeficiency UK, https://www.immunodeficiencyuk.org/immunodeficiency/secondary-immunodeficiency/.
- “Overview on Urinary Tract Infection in Pregnancy.” Medscape, https://emedicine.medscape.com/article/335055-overview?form=fpf#a5.
- Springer Nature. “Secondary Immunodeficiencies.” SpringerLink, Springer, [insert exact Springer URL if required].
Agondi, Rosana C., et al. “Can Patients with Common Variable Immunodeficiency Have Allergic Rhinitis?” American Journal of Rhinology & Allergy, vol. 27, no. 2, 2013, pp. 79–83. PubMed, https://pubmed.ncbi.nlm.nih.gov/23562193/. https://doi.org/10.2500/ajra.2013.27.3855.
Athni, Tejas S., and Sara Barmettler. “Hypogammaglobulinemia, Late-Onset Neutropenia, and Infections Following Rituximab.” Annals of Allergy, Asthma & Immunology, Jan. 2023. https://doi.org/10.1016/j.anai.2023.01.018.
Boyle, J. M., and R. H. Buckley. “Population Prevalence of Diagnosed Primary Immunodeficiency Diseases in the United States.” Journal of Clinical Immunology, vol. 27, no. 5, 2007, pp. 497–502. https://doi.org/10.1007/s10875-007-9103-1.
Brito, Veronica, and Michael S. Niederman. “Pneumonia Complicating Pregnancy.” Clinics in Chest Medicine, vol. 32, no. 1, Mar. 2011, pp. 121–132. https://doi.org/10.1016/j.ccm.2010.10.004.
Chaemsaithong, Piya, et al. “First Trimester Preeclampsia Screening and Prediction.” American Journal of Obstetrics and Gynecology, vol. 226, no. 2, 2022, pp. S1071–S1097.e2. https://doi.org/10.1016/j.ajog.2020.07.020.
Collins, Gary S., et al. “Evaluation of Clinical Prediction Models (Part 1): From Development to External Validation.” BMJ, vol. 384, 2024, e074819. https://doi.org/10.1136/bmj-2023-074819.
Cuadrado, M. J., et al. “Immunoglobulin Abnormalities Are Frequent in Patients with Lupus Nephritis.” BMC Rheumatology, vol. 3, no. 1, 2019. https://doi.org/10.1186/s41927-019-0079-2.
Cunningham-Rundles, C. “Key Aspects for Successful Immunoglobulin Therapy of Primary Immunodeficiencies.” Clinical & Experimental Immunology, vol. 164, 2011, pp. 16–19. https://doi.org/10.1111/j.1365-2249.2011.04390.x.
Cunningham-Rundles, Charlotte. “How I Treat Common Variable Immune Deficiency.” Blood, vol. 116, no. 1, 2010, pp. 7–15. https://doi.org/10.1182/blood-2010-01-254417.
“Fmf-Website.” The Fetal Medicine Foundation, 2026, https://new.fetalmedicine.org/website/#/calculators.
Ghouri, Flavia, et al. “Urinary Tract Infections and Antibiotic Use in Pregnancy—Qualitative Analysis of Online Forum Content.” BMC Pregnancy and Childbirth, vol. 19, no. 1, 2019. https://doi.org/10.1186/s12884-019-2451-z.
Gomes, Catarina Frias, et al. “Gastrointestinal Diseases during Pregnancy: What Does the Gastroenterologist Need to Know?” Annals of Gastroenterology, vol. 31, no. 4, 2018, pp. 385–394. https://doi.org/10.20524/aog.2018.0264.
Habak, Patricia J., and Jr. Griggs. “Urinary Tract Infection in Pregnancy.” StatPearls, StatPearls Publishing, 2024. https://www.ncbi.nlm.nih.gov/books/NBK537047/.
Higuera, Valencia. “Sinus Infection While Pregnant: Prevent and Treat.” Healthline, 17 May 2018, https://www.healthline.com/health/pregnancy/sinus-infection.
Iftikhar, Noreen. “What Stomach Viruses Can You Get in Pregnancy and How Are They Treated?” Healthline, 29 Aug. 2020, https://www.healthline.com/health/pregnancy/stomach-virus-while-pregnant.
Jelena Kornej, et al. “Renal Dysfunction, Stroke Risk Scores (CHADS2, CHA2DS2-VASc, and R2CHADS2), and the Risk of Thromboembolic Events after Catheter Ablation of Atrial Fibrillation.” Circulation: Arrhythmia and Electrophysiology, vol. 6, no. 5, 2013, pp. 868–874. https://doi.org/10.1161/circep.113.000869.
Khalid, Osama M., et al. “A Prospective Study of Acute Sinusitis, Clinical Features and Modalities of Management in Adults, Sudan.” The Egyptian Journal of Otolaryngology, vol. 38, no. 1, 2022, p. 129. https://doi.org/10.1186/s43163-022-00316-9.
Ma Pilar Llobet, et al. “Common Variable Immunodeficiency: 20-Year Experience at a Single Centre.” Pediatric Allergy and Immunology, vol. 20, no. 2, 2009, pp. 113–118. https://doi.org/10.1111/j.1399-3038.2008.00744.x.
Marasco, Carolina, et al. “Management of Common Variable Immunodeficiency by Subcutaneous IgG Self-Administration during Pregnancy: A Case Report.” Clinical Case Reports, vol. 5, no. 8, 2017, pp. 1309–1311. https://doi.org/10.1002/ccr3.692.
Markham, Sarah. “Patient Perspective on Predictive Models in Healthcare: Translation into Practice, Ethical Implications and Limitations.” BMJ Health & Care Informatics, vol. 32, no. 1, 2025, e101153. https://doi.org/10.1136/bmjhci-2024-101153.
Notarangelo, Luigi D., et al. “Primary Immunodeficiencies: 2009 Update.” Journal of Allergy and Clinical Immunology, vol. 124, no. 6, 2009, pp. 1161–1178. https://doi.org/10.1016/j.jaci.2009.10.013.
Odnoletkova, Irina, et al. “The Burden of Common Variable Immunodeficiency Disorders: A Retrospective Analysis of the European Society for Immunodeficiency Registry Data.” Orphanet Journal of Rare Diseases, vol. 13, no. 1, 2018. https://doi.org/10.1186/s13023-018-0941-0.
Park, Joon H., et al. “Perspectives on Common Variable Immune Deficiency.” Annals of the New York Academy of Sciences, vol. 1246, no. 1, 2011, pp. 41–49. https://doi.org/10.1111/j.1749-6632.2011.06338.x.
Pavan-Ramos, Tatiane, et al. “IgG Serum Levels in CVID Patients during Pregnancy.” World Allergy Organization Journal, vol. 8, 2015, A157. https://doi.org/10.1186/1939-4551-8-s1-a157.
Pourshahnazari, Persia, et al. “Secondary Immunodeficiency.” Allergy, Asthma & Clinical Immunology, vol. 20, no. S3, 2025. https://doi.org/10.1186/s13223-024-00925-4.
Searight, Frederick T., et al. “Otitis Media with Effusion.” StatPearls, StatPearls Publishing, 2023. https://www.ncbi.nlm.nih.gov/books/NBK538293/.
Shah, Sonal N., et al. “Does This Child Have Pneumonia?” JAMA, vol. 318, no. 5, 2017, p. 462. https://doi.org/10.1001/jama.2017.9039.
Srinivasa, Bharat T., et al. “Adult Primary Immune Deficiency: What Are We Missing?” The American Journal of Medicine, vol. 125, no. 8, 2012, pp. 779–786. https://doi.org/10.1016/j.amjmed.2012.02.015.
Tudor Fleșeriu, et al. “Maternal HIV Infection and Antiretroviral Therapy in Pregnancy: Implications for Vertical Transmission, Fetal Safety, and Long-Term Infant Outcomes.” Pathogens, vol. 14, no. 8, 2025, p. 818. https://doi.org/10.3390/pathogens14080818.
Wood, Philip M. “Primary Antibody Deficiency Syndromes.” Current Opinion in Hematology, vol. 17, no. 4, 2010, pp. 356–361. https://doi.org/10.1097/moh.0b013e328338f69e.
Yilma, Addis, et al. “HIV/Tuberculosis Coinfection in Pregnancy and the Postpartum Period.” Journal of Clinical Medicine, vol. 12, no. 19, 2023, p. 6302. https://doi.org/10.3390/jcm12196302.
Zainaldain, Hamed, et al. “Infectious Complications Reporting in Common Variable Immunodeficiency: A Systematic Review and Meta-Analysis.” Oman Medical Journal, vol. 35, no. 4, 2020, e157. https://doi.org/10.5001/omj.2020.64.
Bustamante, Jean G., and Mayank Singhal. “Antiphospholipid Syndrome (Antiphospholipid Antibody Syndrome, APS, APLS).” StatPearls, StatPearls Publishing, 2019. https://www.ncbi.nlm.nih.gov/books/NBK430980/.
Hubben, Anne, and Keith R. McCrae. “How to Diagnose and Manage Antiphospholipid Syndrome.” Hematology, vol. 2023, no. 1, 2023, pp. 606–613. https://doi.org/10.1182/hematology.2023000493.
Singh, Megha, et al. “Autoimmune Diseases and Adverse Pregnancy Outcomes: An Umbrella Review.” BMC Medicine, vol. 22, no. 1, 2024. https://doi.org/10.1186/s12916-024-03309-y.
Acknowledgement
Thank you to our mentors, Tatiana Kalashnikova MD, PhD; Haisa Osmanli PhD , Ruzia Ramazanova MD, for working with us and mentoring the creation of Immunimama. Artificial intelligence was used only for the visuals (one in problem section, and first one in the method) to help viewers interpret our project.